The woman, who was in her 90s, had lived for several years at the Ecumen
Sunrise nursing home in Two Harbors, Minn., where the staff had grown accustomed
to her grimaces and wordless cries. She took a potent cocktail of three
psychotropic drugs: Ativan for anxiety and the antipsychotic Risperdal to calm
her, plus an antidepressant. In all the time she’d lived at Sunrise, she hadn’t
spoken. It wasn’t clear whether she could recognize her children when they came
to visit.
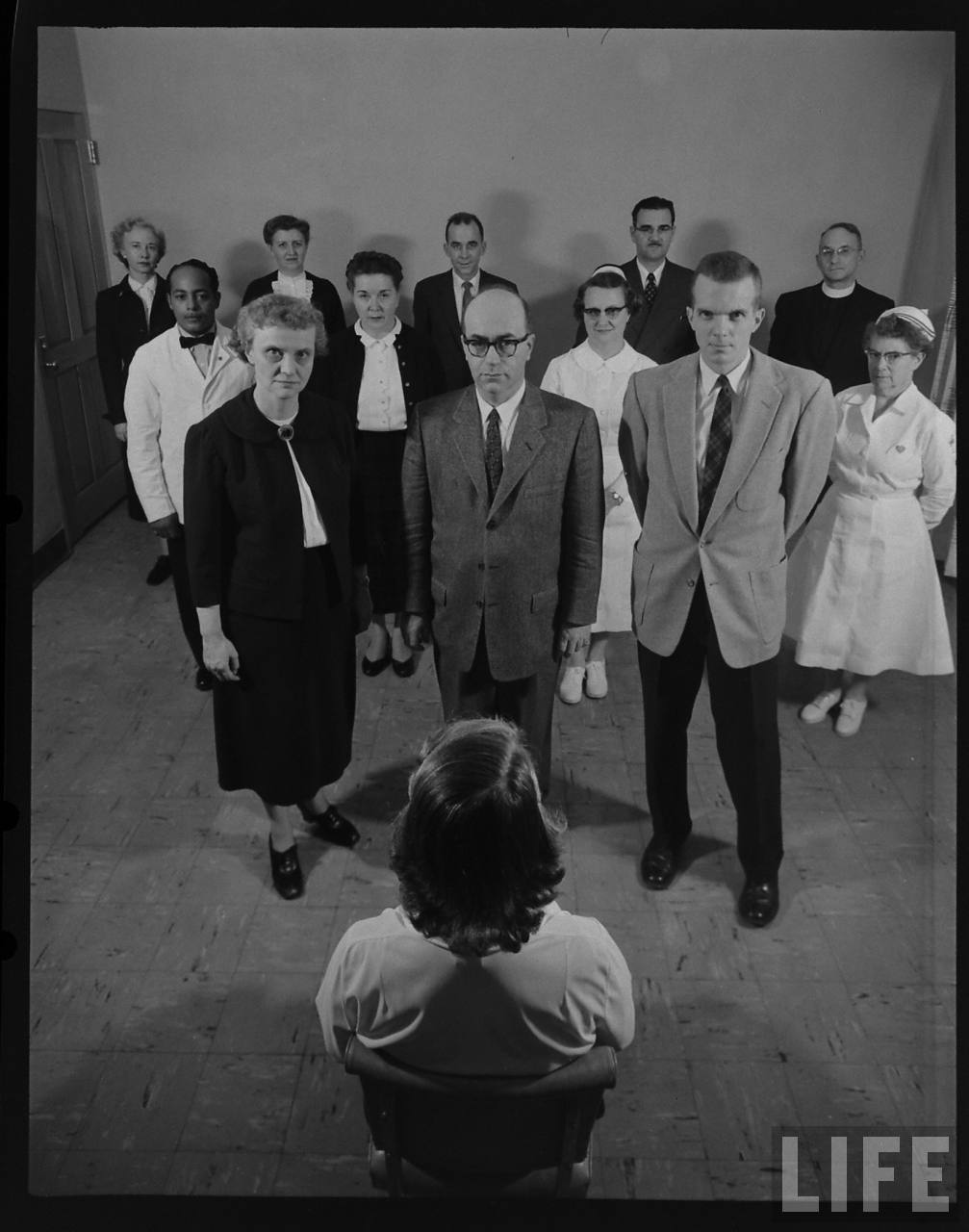
Belinda Day Saylor Eva Lanigan, right, director of nursing at the Ecumen nursing
home in Two Harbors, Minn., with a resident, Marjorie Labrie, 94.The Two Harbors
home happened to be where Ecumen, which operates 16 nonprofit Minnesota nursing
homes, was preparing an experiment to see if behavioral rather than
pharmacological approaches could help wean residents off antipsychotic
medications. They called it the Awakenings program.
“What’s people’s biggest fear? Being a ‘zombie’ in a nursing home,” said Laurel
Baxter, the Awakenings project manager.
Any visitor can see what she means. Even in quality nursing homes, some
residents sit impassively in wheelchairs or nod off in front of televisions,
apparently unable to interact with others or to summon much interest in their
lives. Nursing home reformers and regulators have long believed that this
disengagement results in part from the overuse of psychotropic medication to
quell the troublesome behaviors that can accompany dementia — yelling,
wandering, aggression, resisting care. For nearly 25 years, federal law has
required that psychotropic drugs (which critics call “chemical restraints”) be
used only when necessary to ensure the safety of a resident or those around her.
The drugs can cause serious side effects. Since 2008, the Food and Drug
Administration has required a so-called black box warnings on their packaging,
cautioning that they pose an increased mortality risk for elderly patients.
Nevertheless, a national survey reported that in 2004 about a quarter of nursing
home residents were receiving antipsychotic drugs. (Among the antipsychotic
drugs most commonly used in nursing homes are Risperdal, Seroquel and Zyprexa.)
Though they may be prescribed less frequently following the F.D.A.’s warnings,
these drugs are still overused in long-term care, said Dr. Mark Lachs, chief of
geriatrics at Weill Cornell Medical College. And once the pills are prescribed,
residents keep taking them. “They get perpetualized, like insulin,” he told me,
even though the behaviors they’re meant to soothe may wane anyway as dementia
progresses.
“If a place is understaffed, if it takes particularly unruly patients, you can
see how it happens,” Dr. Lachs added. “Behavioral interventions are far more
time-consuming than giving a pill.”
Nevertheless, Ecumen’s Awakenings project emphasizes nondrug responses.
“Medications have a place, but that shouldn’t be the first thing you try,” said
Eva Lanigan, director of nursing at the Two Harbors facility.
So the home trained its entire staff (housekeepers, cooks, dining room servers,
everyone) in a variety of tools to calm and reassure its 55 residents: exercise,
activities, music, massage, aromatherapy. It taught people the kind of
conversation known as “redirecting” — listening to elders and responding to them
without insisting on facts that those with dementia can’t absorb or won’t
recall.
“The hands-on, caring part is the most important,” Ms. Lanigan said. “Sometimes,
people just want a hug. You sit and hold their hand.”
At the same time, consulting with a geriatric psychiatrist and a pharmacist, the
home began gradually reducing the doses of antipsychotics and antidepressants
for patients whose families agreed. Among them: the woman with the mysterious
cries.
As Dr. Lachs pointed out, behavioral interventions are labor-intensive. Two
Harbors hired an additional nurse to oversee those efforts, and Ms. Lanigan was
available to answer staff questions around the clock. Ecumen estimates that
introducing the program to a 60-bed nursing home cost an additional $75,000 a
year for two full-time employees.
The results startled even the believers, however. Every resident on
antipsychotics (about 10) was able to stop taking them, and 30 to 50 percent of
those taking antidepressants also did well without them. When drugs still seemed
necessary, “we tried to reduce them to the lowest dose possible,” Ms. Lanigan
said.
Encouraged, Ecumen has introduced the Awakenings program to its 15 other nursing
homes, using a $3.8 million, three-year grant from the state of Minnesota. “I
believe we may learn that spending a little time now with a resident, preventing
the use of psychiatric medications and their side effects, you’ll save time and
money in the long run,” said Ms. Baxter, the project manager. “I’m optimistic.”
Of course, you can’t tell how well nondrug approaches work based on one
facility’s outcomes. “We know how to reduce behavior problems and mood issues in
controlled clinical trials,” said Kimberly Van Haitsma, a senior research
scientist at the Polisher Research Institute in Philadelphia. “The actual nuts
and bolts of how do you do this and keep it in place — over not weeks or months,
but years — is a question the field is struggling with.” Turnover among both
staff and residents is high in nursing homes, she pointed out.
But with reduced medications, the woman at the Two Harbors home did seem to
awaken. She was able to speak — haltingly and not always understandably, but
enough to communicate. And what she let Ms. Lanigan know, after years of being
virtually nonverbal, was that she was suffering physical pain, the cause of her
crying out.
It took doctors a while to find effective medications for her nerve condition,
but they were eventually able to make her more comfortable without further
fogging her mind. She stopped taking psychotropic drugs altogether.
None of this can halt dementia; it’s a terminal disease, and it took this
resident’s life last year. But in her final months, she smiled and played
balloon volleyball with other residents and could say she felt fine or was
hungry.
“She engaged more. Her family came to help her eat,” Ms. Lanigan said. “It was a
big change.”
One was a middle-aged man who refused to get into the shower. The other was a
teenager who was afraid to get out.
The man, Leonard, a writer living outside Chicago, found himself completely
unable to wash himself or brush his teeth. The teenager, Ross, growing up in a
suburb of New York, had become so terrified of germs that he would regularly
shower for seven hours. Each received a diagnosis of severe obsessive-compulsive
disorder, or O.C.D., and for years neither felt comfortable enough to leave the
house.
But leave they eventually did, traveling in desperation to a hospital in Rhode
Island for an experimental brain operation in which four raisin-sized holes were
burned deep in their brains.
Today, two years after surgery, Ross is 21 and in college. “It saved my life,”
he said. “I really believe that.”
The same cannot be said for Leonard, 67, who had surgery in 1995. “There was no
change at all,” he said. “I still don’t leave the house.”
Both men asked that their last names not be used to protect their privacy.
The great promise of neuroscience at the end of the last century was that it
would revolutionize the treatment of psychiatric problems. But the first real
application of advanced brain science is not novel at all. It is a precise,
sophisticated version of an old and controversial approach: psychosurgery, in
which doctors operate directly on the brain.
In the last decade or so, more than 500 people have undergone brain surgery for
problems like depression, anxiety, Tourette’s syndrome, even obesity, most as a
part of medical studies. The results have been encouraging, and this year, for
the first time since frontal lobotomy fell into disrepute in the 1950s, the Food
and Drug Administration approved one of the surgical techniques for some cases
of O.C.D.
While no more than a few thousand people are impaired enough to meet the strict
criteria for the surgery right now, millions more suffering from an array of
severe conditions, from depression to obesity, could seek such operations as the
techniques become less experimental.
But with that hope comes risk. For all the progress that has been made, some
psychiatrists and medical ethicists say, doctors still do not know much about
the circuits they are tampering with, and the results are unpredictable: some
people improve, others feel little or nothing, and an unlucky few actually get
worse. In this country, at least one patient was left unable to feed or care for
herself after botched surgery.
Moreover, demand for the operations is so high that it could tempt less
experienced surgeons to offer them, without the oversight or support of research
institutions.
And if the operations are oversold as a kind of all-purpose cure for emotional
problems — which they are not, doctors say — then the great promise could
quickly feel like a betrayal.
“We have this idea — it’s almost a fetish — that progress is its own
justification, that if something is promising, then how can we not rush to
relieve suffering?” said Paul Root Wolpe, a medical ethicist at Emory
University.
It was not so long ago, he noted, that doctors considered the frontal lobotomy a
major advance — only to learn that the operation left thousands of patients with
irreversible brain damage. Many promising medical ideas have run aground, Dr.
Wolpe added, “and that’s why we have to move very cautiously.”
Dr. Darin D. Dougherty, director of the division of neurotherapeutics at
Massachusetts General Hospital and an associate professor of psychiatry at
Harvard, put it more bluntly. Given the history of failed techniques, like
frontal lobotomy, he said, “If this effort somehow goes wrong, it’ll shut down
this approach for another hundred years.”
A Last Resort
Five percent to 15 percent of people given diagnoses of obsessive-compulsive
disorder are beyond the reach of any standard treatment. Ross said he was 12
when he noticed that he took longer to wash his hands than most people. Soon he
was changing into clean clothes several times a day. Eventually he would barely
come out of his room, and when he did, he was careful about what he touched.
“It got so bad, I didn’t want any contact with people,” he said. “I couldn’t hug
my own parents.”
Before turning to writing, Leonard was a healthy, successful businessman. Then
he was struck, out of nowhere, with a fear of insects and spiders. He overcame
the phobias, only to find himself with a strong aversion to bathing. He stopped
washing and could not brush his teeth or shave.
“I just looked horrible,” he said. “I had a big, ugly beard. My skin turned
black. I was afraid to be seen out in public. I looked like a street person. If
you were a policeman, you would have arrested me.”
Both tried antidepressants like Prozac, as well as a variety of other
medications. They spent many hours in standard psychotherapy for
obsessive-compulsive disorder, gradually becoming exposed to dreaded situations
— a moldy shower stall, for instance — and practicing cognitive and relaxation
techniques to defuse their anxiety.
To no avail.
“It worked for a while for me, but never lasted,” Ross said. “I mean, I just
thought my life was over.”
But there was one more option, their doctors told them, a last resort. At a
handful of medical centers here and abroad, including Harvard, the University of
Toronto and the Cleveland Clinic, doctors for years have performed a variety of
experimental procedures, most for O.C.D. or depression, each guided by
high-resolution imaging technology. The companies that make some of the devices
have supported the research, and paid some of the doctors to consult on
operations.
In one procedure, called a cingulotomy, doctors drill into the skull and thread
wires into an area called the anterior cingulate. There they pinpoint and
destroy pinches of tissue that lie along a circuit in each hemisphere that
connects deeper, emotional centers of the brain to areas of the frontal cortex,
where conscious planning is centered.
This circuit appears to be hyperactive in people with severe O.C.D., and imaging
studies suggest that the surgery quiets that activity. In another operation,
called a capsulotomy, surgeons go deeper, into an area called the internal
capsule, and burn out spots in a circuit also thought to be overactive.
An altogether different approach is called deep brain stimulation, or D.B.S., in
which surgeons sink wires into the brain but leave them in place. A
pacemaker-like device sends a current to the electrodes, apparently interfering
with circuits thought to be hyperactive in people with obsessive-compulsive
disorder (and also those with severe depression). The current can be turned up,
down or off, so deep brain stimulation is adjustable and, to some extent,
reversible.
In yet another technique, doctors place the patient in an M.R.I.-like machine
that sends beams of radiation into the skull. The beams pass through the brain
without causing damage, except at the point where they converge. There they burn
out spots of tissue from O.C.D.-related circuits, with similar effects as the
other operations. This option, called gamma knife surgery, was the one Leonard
and Ross settled on.
The institutions all have strict ethical screening to select candidates. The
disorder must be severe and disabling, and all standard treatments exhausted.
The informed-consent documents make clear that the operation is experimental and
not guaranteed to succeed.
Nor is desperation by itself sufficient to qualify, said Richard Marsland, who
oversees the screening process at Butler Hospital in Providence, R.I., which
works with surgeons at Rhode Island Hospital, where Leonard and Ross had the
operation.
“We get hundreds of requests a year and do only one or two,” Mr. Marsland said.
“And some of the people we turn down are in bad shape. Still, we stick to the
criteria.”
For those who have successfully recovered from surgery, this intensive screening
seems excessive. “I know why it’s done, but this is an operation that could make
the difference between life and death for so many people,” said Gerry Radano,
whose book “Contaminated: My Journey Out of Obsessive-Compulsive Disorder”
(Bar-le-Duc Books, 2007), recounts her own suffering and long recovery from
surgery. She also has a Web site, freeofocd.com, where people from around the
world consult with her.
But for the doctors running the programs, this screening is crucial. “If
patients are poorly selected or not followed well, there’ll be an increasing
number of bad outcomes, and the promise of this field will wither away,” said
Dr. Ben Greenberg, the psychiatrist in charge of the program at Butler.
Dr. Greenberg said about 60 percent of patients who underwent either gamma knife
surgery or deep brain stimulation showed significant improvement, and the rest
showed little or no improvement. For this article, he agreed to put a reporter
in touch with one — Leonard — who did not have a good experience.
The Danger of Optimism
The true measure of an operation, medical ethicists say, is its overall effect
on a person’s life, not only on specific symptoms.
In the early days of psychosurgery, after World War II, doctors published scores
of papers detailing how lobotomy relieved symptoms of mental distress. In 1949,
the Portuguese neurologist Egas Moniz won the Nobel Prize in medicine for
inventing the procedure.
But careful follow-up painted a darker picture: of people who lost motivation,
who developed the helpless indifference dramatized by the post-op rebel McMurphy
in Ken Kesey’s novel “One Flew Over the Cuckoo’s Nest,” played by Jack Nicholson
in the 1975 movie.
The newer operations pinpoint targets on specific, precisely mapped circuits,
whereas the frontal lobotomy amounted to a crude slash into the brain behind the
eyes, blindly mangling whatever connections and circuits were in the way. Still,
there remain large gaps in doctors’ understanding of the circuits they are
operating on.
In a paper published last year, researchers at the Karolinska Institute in
Sweden reported that half the people who had the most commonly offered
operations for obsessive-compulsive disorder showed symptoms of apathy and poor
self-control for years afterward, despite scoring lower on a measure of O.C.D.
severity.
“An inherent problem in most research is that innovation is driven by groups
that believe in their method, thus introducing bias that is almost impossible to
avoid,” Dr. Christian Ruck, the lead author of the paper, wrote in an e-mail
message. The institute’s doctors, who burned out significantly more tissue than
other centers did, no longer perform the operations, partly, Dr. Ruck said, as a
result of his findings.
In the United States, at least one patient has suffered disabling brain damage
from an operation for O.C.D. The case led to a $7.5 million judgment in 2002
against the Ohio hospital that performed the procedure. (It is no longer offered
there.)
Most outcomes, whether favorable or not, have had less remarkable immediate
results. The brain can take months or even years to fully adjust after the
operations. The revelations about the people treated at Karolinska “underscore
the importance of face-to-face assessments of adverse symptoms,” Dr. Ruck and
his co-authors concluded.
The Long Way Back
Ross said he felt no difference for months after surgery, until the day his
brother asked him to play a video game in the basement, and down the stairs he
went.
“I just felt like doing it,” he said. “I would never have gone down there
before.”
He said the procedure seemed to give the psychotherapy sessions a chance to
work, and last summer he felt comfortable enough to stop them. He now spends his
days studying, going to class, playing the odd video game to relax. He has told
friends about the operation, he said, “and they’re O.K. with it — they know the
story.”
Leonard is still struggling, for reasons no one understands. He keeps odd hours,
working through most nights and sleeping much of the day. He is not unhappy, he
said, but he has the same aversion to washing and still lives like a hermit.
“I still don’t know why I’m like this, and I would still try anything that could
help,” he said. “But at this point, obviously, I’m skeptical of the efficacy of
surgery, at least for me.”
Ms. Radano, who wrote the book about her recovery, said the most important thing
about the surgery was that it gave people a chance. “That’s all people in this
situation want, and I know because I was there,” she said while getting into her
car on a recent afternoon.
On the passenger seat was a container of decontaminating hand wipes. She pointed
and laughed. “See? You’re never completely out.”
In the
'50s, disabled children
often disappeared into state institutions.
Now, one
family seeks its lost son.
May 31,
2008; Page A1
The Wall Street Journal
By CLARE ANSBERRY
PORTLAND,
Ore. -- Tom and Betty West committed their mentally disabled son to a state
institution. His name was Richard, and he was three years old. It was 1959. The
massive complex was remote and family ties not encouraged. The state eventually
moved Richard to a different facility without informing the Wests of the
location. Four decades passed without a family member laying eyes on Richard.
As they
entered their 80s, the Wests thought increasingly about Richard, the fifth of
their eight children. How was he? Where did he live? Mr. West wanted to make
sure that, following his death, some of his pension flowed to Richard.
State officials rejected Mr. West's request for information, calling Richard's
whereabouts private. The Wests hired an attorney who ran into the same
roadblocks. "At that point, I thought there is nothing more I could do," says
Mr. West, a retired dam builder who is 87.
The Wests belong to a generation of parents who decades ago relinquished their
disabled children, usually at the urging of physicians or other authorities.
From the 1930s into the 1960s, tens of thousands of these children entered state
facilities, which offered services that local communities lacked. Many never saw
their families again.
"Fifty years ago, families were often advised to place their child in an
institution, and basically told that, for the good of the child and family, to
forget that the person existed," says Charlie Lakin, project director of the
Research and Training Center on Community Living at the University of Minnesota.
Back in the
'60s, an Oregon family put their mentally disabled child in a public
institution, and he eventually became a ward of the state. Recently, the family
tracked him to a small group home and hope to retie lost bonds. (May 31)
Half a century later, that old policy is still haunting families across America.
Middle-aged siblings want to find their absent younger brother or sister before
it is too late. Aging parents wish they knew what became of their child. Cousins
and nieces wonder about relatives known only by name and family lore.
Yet even as greater acceptance and inclusion greet today's mentally disabled
children, many of yesterday's remain lost. Privacy laws can prevent families
from finding their loved ones. In some cases, facilities have closed, scattering
residents into group homes and apartments without family notification. About 40%
of residents of large state institutions have no family contact, surveys have
shown.
Efforts to help restore lost connections are surfacing. In 2005, Oregon passed
legislation and adopted a procedure to make it easier for relatives to track
down people who were institutionalized. A dozen other states are studying its
approach.
Last summer, Arc, a national advocacy group for the developmentally disabled,
created a registry where people can list who they are trying to find. About 290
families have registered, from nearly every state. But a match can be made only
if both sides register. Of the 86 disabled adults who have registered, none have
been matched to registered families. Among those searching is a 50-year-old
woman who learned only in adulthood about the existence of her developmentally
disabled twin sister, says Arc.
'Brother
Was in Fairview'
One evening in 2005, a television news channel in Portland interviewed a man
named Jeff Daly about the discovery of his developmentally disabled sister,
Molly, who had been living at Oregon's Fairview home.
Watching TV that night was Jeff West, the youngest sibling of Richard West. Born
after Richard left their family home, Jeff West had never met his brother. But
he knew all about him, including the name of the first institution Richard had
entered. Turning to his wife as they watched that interview, Jeff West said: "My
brother was in Fairview."
At the time
she became pregnant with their fifth child in 1955, Betty and Tom West lived in
a three-bedroom house in The Dalles, Ore. The pregnancy went smoothly, but the
delivery didn't. Richard was blue at birth and immediately put on oxygen, then
sent home with assurances that he was fine.
He rarely cried. But as months passed, he didn't roll over or crawl. He showed
little emotion or recognition. If Mrs. West walked out of the room, he didn't
protest. His older brothers played around him. "He seemed like he was in his own
little world," recalls his older brother Steve.
Mrs. West read to him and repeated basic words, hoping he would catch on. Once,
she thought he said "Mama," but he never said it again. When she started giving
him solid food, he choked. At age two, he weighed 17 pounds. "I knew there was
something wrong, but I couldn't pinpoint it," she says.
At monthly checkups, she relayed her concerns to her doctor, who said Richard
was fine. As months passed without progress, she insisted something was wrong.
Tired of her questions, the doctor told her not to come back, she says.
Second
Opinion
Mrs. West found a new physician who examined Richard and concluded he was
severely mentally retarded. The physician explained that Richard might learn to
walk but would never talk. He would always have the mentality of a
three-year-old and need 24-hour care. "It was a relief knowing it wasn't my
imagination" or fault, says Mrs. West.
Soon pregnant again, Mrs. West became overwhelmed at the thought of caring for a
newborn and a mentally disabled toddler, along with four older kids. The
community offered no programs to help Richard. Having come from North Dakota,
the Wests had no family nearby. "I didn't know what to do," says Mrs. West.
She asked her doctor. Gently, he told Mrs. West it would be better for Richard
and everyone else if he was institutionalized. "You have to think of the other
kids," she remembers the physician telling her.
She was numb. It went against everything the young couple believed. They had
built a close family. They had come from close families.
In the end, they felt they had no other option. After Richard received an
official diagnosis of "idiot" and "marked mental retardation," the Wests
reluctantly agreed to send him 130 miles away to Oregon Fairview Home near
Salem. A sprawling complex of dormitories and agricultural operations, Fairview
was crowded with a wave of baby boomers with developmental disabilities. At
mealtime, nurses lined children in high chairs against the wall, feeding the
younger ones and taping forks into the hands of older children to encourage use
of utensils.
Black-and-White Film
An old black-and-white film called "In Our Care" describes Fairview, showing a
porch crowded with children clapping and rolling a ball. "This child spends most
of her time tearing paper into shreds," the narrator says.
The day Richard left for Fairview, Mrs. West packed his clothes and dressed him
in his best outfit -- a white blazer with a crest on the pocket and dark shorts.
She and her husband told the other children Richard was going to a place where
he could get special care. "We kind of knew he had a problem that our mother
just couldn't take care of," says the oldest, Tom Jr., who was 11 at the time.
At the front office, an administrator recommended that Mr. and Mrs. West kiss
Richard goodbye and leave quickly. "It was a terribly difficult day," says Betty
West.
To visit Richard, the Wests had to make appointments. They tried to see him at
least once in the summer, bringing along the other children. Richard didn't seem
to recognize them but held their hands as they played Ring around the Rosie. His
younger sister Barbara West remembers the smell of antiseptic and wondering why
her older brother slept in a crib when she didn't.
One afternoon, when Richard was about 8 years old, his parents were walking
hand-in-hand with him down the sidewalk. An older woman approached and held her
hands out. Richard wriggled free and ran into the woman's outstretched arms. He
hugged her, showing affection he had never shown his family. Betty remembers
crying and telling her husband it was time to let go.
'Let Him
Be'
"He has someone who loves him here. She makes him happy. We need to let him be,"
she recalls saying.
They continued to send him clothing but never went back to visit.
"He didn't know us," says Mrs. West.
"That was the only thing that made it bearable," says her husband.
In the West home, Richard became a powerful memory. The youngest child, Jeff,
saw various photographs of the brother he'd never met -- Richard on the floor
with his older brothers, Richard at the pool with their mother, Richard dressed
up the day he went to Fairview. His parents had told Jeff why Richard didn't
live at home. "They never shied away from talking about him," says Jeff.
No
Forwarding Address
None of the children pressed their parents to find out how Richard was doing,
although privately they wondered. "Anytime the family was together at Christmas
or Thanksgiving, I would think how we used to play around him on the floor,"
says his older brother Bob.
In the 1980s, the state informed the Wests that Richard was being moved a couple
hundred miles east to another state facility. A few years later, the Wests
received a letter saying Richard was being placed in a smaller residence. The
letter didn't say where. The Wests felt they lacked standing to ask because
their son was a ward of the state.
He had, in fact, been transferred to a group home in Baker City, about 300 miles
away. There, workers wondered about Richard's family. "Do they know he exists?
Do they care?" says caregiver Tracy Hylton. "Many families don't want to have
contact, and when there isn't any contact, we have to assume that is the case."
The turning point came the evening that Jeff West saw the television interview
with Mr. Daly, the Oregon man who had found his long-lost mentally disabled
sister. Suddenly, Jeff West was struck with the desire to find Richard.
Other siblings, however, were apprehensive. "Do you really want to do that?"
brother Larry remembers saying. "Are you going to bring up things that are
hurtful?"
Debby Peery, the second-youngest, wondered what their responsibility might be
and how others would react.
"I was a little nervous about what the caretakers would think of us suddenly
showing up after 40 years," she says. "But I was also excited."
All worried about their parents. "I didn't know how much guilt they carried,"
says Jeff West. At that point, Jeff didn't know his parents had recently and
unsuccessfully tried to find Richard so that he could receive Mr. West's
pension.
When asked about tracking down his disabled son, the elderly Mr. West responded,
"Go for it."
40 Years
Later
A flurry of phone calls followed. Jeff West talked to Mr. Daly, who gave him
phone numbers of agencies with group homes. One was in Baker City. Jeff West
provided his parents' Social Security numbers and Richard's date of birth to
verify he was family. The woman at the group home said Richard was there.
Weeks later, the family met with Richard for the first time in 40 years. His
caregivers, Ms. Hylton and Carrie Baird, drove Richard to the home of a sibling.
They worried whether the West family would take Richard away from his group
home, where he was comfortable and loved. "It would have been hard for us if he
left," says Ms. Hylton.
Likewise, Mr. and Mrs. West felt anxious, not knowing whether Richard would want
to see them or be angry. "I didn't know how he would take to us," says Mr. West.
Richard walked in, holding a Sponge Bob Square pants book with buttons that
played songs. His parents sat on one couch. He sat on another, next to Ms.
Hylton and Ms. Baird, holding their hands. He looked around the room, his face
registering no apparent emotion. Mrs. West held back the urge to hold him. "I
would have loved to given him a hug," she says. "But they said don't touch him
because he won't like it."
Dates at
McDonald's
Over lunch and through the afternoon, the Wests listened to Ms. Hylton and Ms.
Baird describe how Richard loves music, does his own laundry, washes dishes,
mows the lawn and sets the table. He has a job refilling ink cartridges. And a
girlfriend: On dates to McDonalds they eat apple pie. Always known to his family
as Ricky, he now preferred to be called Richard.
The Wests told stories about Richard's younger years and their struggles to help
him. Richard grew restless and pressed a button on his book that is his signal
to leave. He walked outside and got in the van.
Mr. and Mrs. West thanked Ms. Hylton and Ms. Baird for taking good care of
Richard. The Wests say it eased their minds to see Richard healthy and seemingly
content.
A few months after visiting Richard, Jeff West received Richard's signed
permission to look at his records at Oregon's Department of Human Services
office. Going through them helped the family piece together the unknown part of
Richard's life. Some was reassuring. Some wasn't.
At Fairview, Richard learned things his parents never thought possible. By 12,
he could dress, feed himself, catch a ball, fold pajamas and fish. He had
friends and foster grandparents who took him out for ice cream. At 16, Richard
taught himself to whistle. He loved Volkswagens and was sometimes found sitting
in one in the Fairview parking lot.
Then there were glimpses of what they envisioned institutional life would be
like. Over the years, Richard would run away and get in trouble for hitting. He
was often put on Thorazine to sedate him.
Like Oliver
Twist
Most troubling were the annual photographs of him behind a board saying,
"Richard Alan West, Case 5727." In the photos, his face is thin and
expressionless. The images reminded his parents of orphans begging for gruel in
Oliver Twist. "That doesn't look like a very nice life," says Mr. West.
The records also contained references to the times that the Wests visited
Richard. The documents said Richard had become visibly upset and withdrawn
following their departure -- suggesting that he had known them better than they
had realized. "These were things we didn't know," says Mr. West.
Now, Richard receives regular calls, letters, McDonald's gift certificates and
visits from his family. Last summer, the family drove four cars to Richard's
home. This summer, the Wests are hoping to have Richard home for a family
reunion.
Mrs. West sends Richard towels and sweatshirts embroidered with his name. When
getting dressed in the morning, Richard selects the same shirts repeatedly --
the ones his mother sent. "He knows it came from his family, and it means
something," says Ms. Hylton.
The
family's dark secret
until her brother, President Kennedy,
acknowledged her
Tuesday 11
January 2005
00.03 GMT
The Guardian
Sue Woodman
This article was first published
on guardian.co.uk at 00.03 GMT
on Tuesday 11
January 2005.
It was last updated at 00.03 GMT
on Tuesday 11 January 2005.
From early
in childhood, it was evident that Rosemary Kennedy, who has died aged 86, had
developmental problems. Rosemary - Rose or Rosie to her family - was sister to
John F Kennedy, and the third of nine children of the privileged, wealthy Boston
family of Joseph and Rose Kennedy.
Rosemary
was lobotomised at the age of 23, and spent her adult life in institutional
care. Her plight led her younger sister, Eunice Kennedy Shriver, to champion
mental health projects, and to found the Special Olympics in 1968 to celebrate
the prowess of mentally disabled athletes.
Rosemary had been slow to walk and talk, and had neither the academic nor the
athletic skills of her siblings. An IQ test showed mental retardation. But her
ambitious father, Joe, kept her condition secret, not just from the public, but
from friends and distant family as well. He believed the truth could harm his
sons' political aspirations and tarnish his family's shining aura.
The Kennedys had Rosemary schooled at home by governesses and nuns, and allowed
her to attend balls and parties if accompanied by her brothers. Diaries from
1936 and 1938 describe the tea parties, dress fittings and social visits that
were part of Rosemary's life, as well as her visit to the White House in the era
of President Franklin D Roosevelt.
When Rosemary's mood swings and temper became hard to control, the family moved
her to a convent. She began to sneak out at night, and the family feared she
might come to harm - or get pregnant. Her father was desperate for a solution.
It was recommended to him in 1941 that Rosemary have a prefrontal lobotomy,
which involved cutting fibres in the brain, an operation intended to calm
severely mentally ill patients. This procedure had been performed on perhaps
350-500 people by then, all but one of them older and sicker than Rosemary.
The lobotomy did not help. In fact, it caused Rosemary to regress into a
childlike state in which she sat for hours staring at the walls. Her rage stayed
unabated. She was then sent to an institution where her father never visited
her. And whenever her mother came, Rosemary refused to acknowledge her.
Rosemary was not referred to again in public until 1960, when her brother John
became president. A statement from the National Association for Retarded
Children revealed that he had "a mentally retarded sister who is in an
institution in Wisconsin".
Rosemary lived at the St Coletta School for Exceptional Children in Jefferson,
Wisconsin, from 1949 until her death. Her home was a house on the school
grounds, which had been specially built for her and two nurses.
Rosemary's most devoted champion was Eunice, who took over her care after their
mother's stroke in 1983. Eunice visited Rosemary regularly and brought her home
for visits.
Eunice persuaded her father to use the resources of the Joseph P Kennedy
Foundation to support causes for the mentally ill. Over the decades, the Kennedy
family have funded research and built several facilities. Eunice travelled
widely to promote the cause, even conferring with President de Gaulle, who had a
retarded child.
A Kennedy family statement, announcing Rosemary's death, called her "a lifelong
jewel to every member of our family... From her earliest years, her mental
retardation was a continuing inspiration to each of us and a powerful source of
our family's commitment to do all we can to help all persons with disabilities
live full and productive lives."
Eunice, 83, and Rosemary's other sisters Patricia, 80, and Jean, 76, were with
her at her death, as was her surviving brother, Senator Edward Kennedy, 72.