|
History > 2006 > USA > Health (IV)
NYT
October 2, 2006
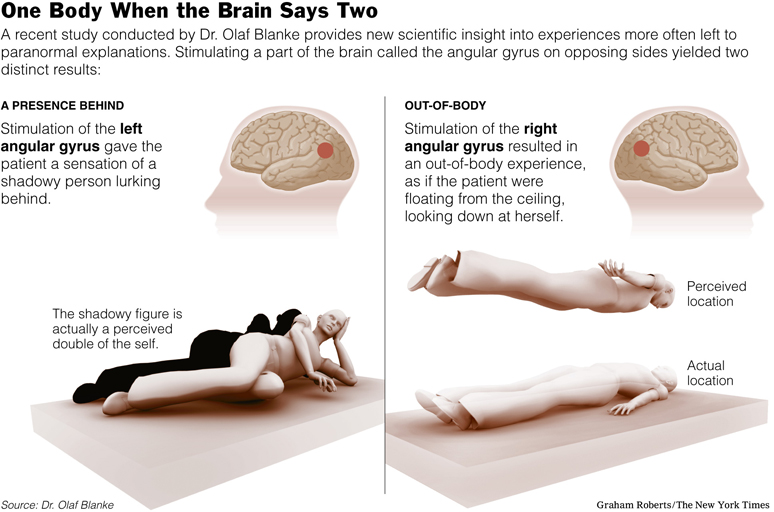
Out-of-Body Experience? Your Brain Is to Blame
NYT 3.10.2006
http://www.nytimes.com/2006/10/03/health/psychology/03shad.html
One for the Ages:
A Prescription That May
Extend Life
October 31, 2006
The New York Times
By MICHAEL MASON
How depressing, how utterly unjust, to be the
one in your social circle who is aging least gracefully.
In a laboratory at the Wisconsin National Primate Research Center, Matthias is
learning about time’s caprice the hard way. At 28, getting on for a rhesus
monkey, Matthias is losing his hair, lugging a paunch and getting a face full of
wrinkles.
Yet in the cage next to his, gleefully hooting at strangers, one of Matthias’s
lab mates, Rudy, is the picture of monkey vitality, although he is slightly
older. Thin and feisty, Rudy stops grooming his smooth coat just long enough to
pirouette toward a proffered piece of fruit.
Tempted with the same treat, Matthias rises wearily and extends a frail hand.
“You can really see the difference,” said Dr. Ricki Colman, an associate
scientist at the center who cares for the animals.
What a visitor cannot see may be even more interesting. As a result of a simple
lifestyle intervention, Rudy and primates like him seem poised to live very
long, very vital lives.
This approach, called calorie restriction, involves eating about 30 percent
fewer calories than normal while still getting adequate amounts of vitamins,
minerals and other nutrients. Aside from direct genetic manipulation, calorie
restriction is the only strategy known to extend life consistently in a variety
of animal species.
How this drastic diet affects the body has been the subject of intense research.
Recently, the effort has begun to bear fruit, producing a steady stream of
studies indicating that the rate of aging is plastic, not fixed, and that it can
be manipulated.
In the last year, calorie-restricted diets have been shown in various animals to
affect molecular pathways likely to be involved in the progression of
Alzheimer’s disease, diabetes, heart disease, Parkinson’s disease and cancer.
Earlier this year, researchers studying dietary effects on humans went so far as
to claim that calorie restriction may be more effective than exercise at
preventing age-related diseases.
Monkeys like Rudy seem to be proving the thesis. Recent tests show that the
animals on restricted diets, including Canto and Eeyore, two other rhesus
monkeys at the primate research center, are in indisputably better health as
they near old age than Matthias and other normally fed lab mates like Owen and
Johann. The average lifespan for laboratory monkeys is 27.
The findings cast doubt on long-held scientific and cultural beliefs regarding
the inevitability of the body’s decline. They also suggest that other
interventions, which include new drugs, may retard aging even if the diet itself
should prove ineffective in humans. One leading candidate, a newly synthesized
form of resveratrol — an antioxidant present in large amounts in red wine — is
already being tested in patients. It may eventually be the first of a new class
of anti-aging drugs. Extrapolating from recent animal findings, Dr. Richard A.
Miller, a pathologist at the University of Michigan, estimated that a pill
mimicking the effects of calorie restriction might increase human life span to
about 112 healthy years, with the occasional senior living until 140, though
some experts view that projection as overly optimistic.
According to a report by the Rand Corporation, such a drug would be among the
most cost-effective breakthroughs possible in medicine, providing Americans more
healthy years at less expense (an estimated $8,800 a year) than new cancer
vaccines or stroke treatments.
“The effects are global, so calorie restriction has the potential to help us
identify anti-aging mechanisms throughout the body,” said Richard Weindruch, a
gerontologist at the University of Wisconsin who directs research on the
monkeys.
Many scientists regard the study of life extension, once just a reliable
plotline in science fiction, as a national priority. The number of Americans 65
and older will double in the next 25 years to about 72 million, according to
government census data. By then, seniors will account for nearly 20 percent of
the population, up from just 12 percent in 2003.
Earlier this year, four prominent gerontologists, among them Dr. Miller,
published a paper calling for the government to spend $3 billion annually in
pursuit of a modest goal: delaying the onset of age-related diseases by seven
years.
Doing so, the authors asserted, would lay the foundation for a healthier and
wealthier country, a so-called longevity dividend.
“The demographic wave entering their 60s is enormous, and that is likely to
greatly increase the prevalence of diseases like diabetes and heart disease,”
said Dr. S. Jay Olshansky, an epidemiologist at the University of Illinois at
Chicago, and one of the paper’s authors. “The simplest way to positively affect
them all is to slow down aging.”
Science, of course, is still a long way from doing anything of the sort. Aging
is a complicated phenomenon, the intersection of an array of biological
processes set in motion by genetics, lifestyle, even evolution itself.
Still, in laboratories around the world, scientists are becoming adept at
breeding animal Methuselahs, extraordinarily long lived and healthy worms, fish,
mice and flies.
In 1935, Dr. Clive McCay, a nutritionist at Cornell University, discovered that
mice that were fed 30 percent fewer calories lived about 40 percent longer than
their free-grazing laboratory mates. The dieting mice were also more physically
active and far less prone to the diseases of advanced age.
Dr. McCay’s experiment has been successfully duplicated in a variety of species.
In almost every instance, the subjects on low-calorie diets have proven to be
not just longer lived, but also more resistant to age-related ailments.
“In mice, calorie restriction doesn’t just extend life span,” said Leonard P.
Guarente, professor of biology at the Massachusetts Institute of Technology. “It
mitigates many diseases of aging: cancer, cardiovascular disease,
neurodegenerative disease. The gain is just enormous.”
For years, scientists financed by the National Institute on Aging have closely
monitored rhesus monkeys on restricted and normal-calorie diets. At the
University of Wisconsin, where 50 animals survive from the original group of 76,
the differences are just now becoming apparent in the older animals.
Those on normal diets, like Matthias, are beginning to show signs of advancing
age similar to those seen in humans. Three of them, for instance, have developed
diabetes, and a fourth has died of the disease. Five have died of cancer.
But Rudy and his colleagues on low-calorie meal plans are faring better. None
have diabetes, and only three have died of cancer. It is too early to know if
they will outlive their lab mates, but the dieters here and at the other labs
also have lower blood pressure and lower blood levels of certain dangerous fats,
glucose and insulin.
“The preliminary indicators are that we’re looking at a robust life extension in
the restricted animals,” Dr. Weindruch said.
Despite widespread scientific enthusiasm, the evidence that calorie restriction
works in humans is indirect at best. The practice was popularized in diet books
by Dr. Roy Walford, a legendary pathologist at the University of California, Los
Angeles, who spent much of the last 30 years of his life following a
calorie-restricted regimen. He died of Lou Gehrig’s disease in 2004 at 79.
Largely as a result of his advocacy, several thousand people are now on
calorie-restricted diets in the United States, says Brian M. Delaney, president
of the Calorie Restriction Society.
Mike Linksvayer, a 36-year-old chief technology officer at a San Francisco
nonprofit group, embarked on just such a diet six years ago. On an average day,
he eats an apple or some cereal for breakfast, followed by a small vegan dish at
lunch. Dinner is whatever his wife has cooked, excluding bread, rice, sugar and
whatever else Mr. Linksvayer deems unhealthy (this often includes the entrée).
On weekends, he occasionally fasts.
Mr. Linksvayer, 6 feet tall and 135 pounds, estimated that he gets by on about
2,000 to 2,100 calories a day, a low number for men of his age and activity
level, and his blood pressure is a remarkably low 112 over 63. He said he has
never been in better health.
“I don’t really get sick,” he said. “Mostly I do the diet to be healthier, but
if it helps me live longer, hey, I’ll take that, too.”
Researchers at Washington University in St. Louis have been tracking the health
of small groups of calorie-restricted dieters. Earlier this year, they reported
that the dieters had better-functioning hearts and fewer signs of inflammation,
which is a precursor to clogged arteries, than similar subjects on regular
diets.
In previous studies, people in calorie-restricted groups were shown to have
lower levels of LDL, the so-called bad cholesterol, and triglycerides. They also
showed higher levels of HDL, the so-called good cholesterol, virtually no
arterial blockage and, like Mr. Linksvayer, remarkably low blood pressure.
“Calorie restriction has a powerful, protective effect against diseases
associated with aging,” said Dr. John O. Holloszy, a Washington University
professor of medicine. “We don’t know how long each individual will end up
living, but they certainly have a longer life expectancy than average.”
Researchers at Louisiana State University reported in April in The Journal of
the American Medical Association that patients on an experimental low-calorie
diet had lower insulin levels and body temperatures, both possible markers of
longevity, and fewer signs of the chromosomal damage typically associated with
aging.
These studies and others have led many scientists to believe they have stumbled
onto a central determinant of natural life span. Animals on restricted diets
seem particularly resistant to environmental stresses like oxidation and heat,
perhaps even radiation. “It is a very deep, very important function,” Dr. Miller
said. Experts theorize that limited access to energy alarms the body, so to
speak, activating a cascade of biochemical signals that tell each cell to direct
energy away from reproductive functions, toward repair and maintenance. The
calorie-restricted organism is stronger, according to this hypothesis, because
individual cells are more efficiently repairing mutations, using energy,
defending themselves and mopping up harmful byproducts like free radicals.
“The stressed cell is really pulling out all the stops” to preserve itself, said
Dr. Cynthia Kenyon, a molecular biologist at the University of California, San
Francisco. “This system could have evolved as a way of letting animals take a
timeout from reproduction when times are harsh.”
But many experts are unsettled by the prospect, however unlikely, of Americans
adopting a draconian diet in hopes of living longer. Even the current
epidemiological data, they note, do not consistently show that those who are
thinnest live longest. After analyzing decades of national mortality statistics,
federal researchers reported last year that exceptional thinness, a logical
consequence of calorie restriction, was associated with an increased risk of
death. This controversial study did not attempt to assess the number of calories
the subjects had been consuming, or the quality of their diets, which may have
had an effect on mortality rates.
Despite the initially promising results from studies of primates, some
scientists doubt that calorie restriction can ever work effectively in humans. A
mathematical model published last year by researchers at University of
California, Los Angeles, and University of California, Irvine, predicted that
the maximum life span gain from calorie restriction for humans would be just 7
percent. A more likely figure, the authors said, was 2 percent.
“Calorie restriction is doomed to fail, and will make people miserable in the
process of attempting it,” said Dr. Jay Phelan, an evolutionary biologist at the
University of California, Los Angeles, and a co-author of the paper. “We do see
benefits, but not an increase in life span.”
Mice who must scratch for food for a couple of years would be analogous, in
terms of natural selection, to humans who must survive 20-year famines, Dr.
Phelan said. But nature seldom demands that humans endure such conditions.
Besides, he added, there is virtually no chance Americans will adopt such a
severe menu plan in great numbers.
“Have you ever tried to go without food for a day?” Dr. Phelan asked. “I did it
once, because I was curious about what the mice in my lab experienced, and I
couldn’t even function at the end of the day.”
Even researchers who believe calorie restriction can extend life in humans
concede that few Americans are likely to stick to such a restrained diet over a
long period. The aging of the body is the aging of its cells, researchers like
to say. While cell death is hardwired into every organism’s DNA, much of the
infirmity that comes with advancing years is from an accumulation of molecular
insults that, experts contend, may to some degree be prevented, even reversed.
“The goal is not just to make people live longer,” said Dr. David A. Sinclair, a
molecular biologist at Harvard. “It’s to see eventually that an 80-year-old
feels like a 50-year-old does today.”
In a series of studies, Dr. Kenyon, of the University of California, San
Francisco, has created mutant roundworms that live six times longer than normal,
largely because of a mutation in a single gene called daf-2. The gene encodes a
receptor on the surface of cells similar to a receptor in humans that responds
to two important hormones, insulin and the insulin-like growth factor 1 or
IGF-1.
Insulin is necessary for the body to transport glucose into cells to fuel their
operations. Dr. Kenyon and other researchers suggest that worm cells with
mutated receptors may be “tricked” into sensing that nutrients are not
available, even when they are. With its maintenance machinery thereby turned on
high, each worm cell lives far longer — and so does the worm.
Many experts are now convinced that the energy-signaling pathways that employ
insulin and IGF-1 are very involved in fixing an organism’s life span. Some
researchers have even described Type 2 diabetes, which is marked by
insensitivity to the hormone insulin, as simply an accelerated form of aging.
In yeast, scientists have discovered a gene similar to daf-2 called SIR2, that
also helps to coordinate the cell’s defensive response once activated by calorie
restriction or another external stressor. The genes encode proteins called
sirtuins, which are found in both plants and animals.
A mammalian version of the SIR2 gene, called SIRT1, has been shown to regulate a
number of processes necessary for long-term survival in calorie-restricted mice.
Scientists are now trying to develop synthetic compounds that affect the genes
daf-2 and SIRT1.
Several candidate drugs designed to prevent age-related diseases, particularly
diabetes, are on the drawing boards at biotech companies. Sirtris
Pharmaceuticals, in Boston, already has begun testing a new drug in patients
with Type 2 diabetes that acts on SIRT1 to improve the functioning of
mitochondria, the cell’s energy factories.
While an anti-aging pill may be the next big blockbuster, some ethicists believe
that the all-out determination to extend life span is veined with arrogance. As
appointments with death are postponed, says Dr. Leon R. Kass, former chairman of
the President’s Council on Bioethics, human lives may become less engaging, less
meaningful, even less beautiful.
“Mortality makes life matter,” Dr. Kass recently wrote. “Immortality is a kind
of oblivion — like death itself.”
That man’s time on this planet is limited, and rightfully so, is a cultural
belief deeply held by many. But whether an increasing life span affords greater
opportunity to find meaning or distracts from the pursuit, the prospect has
become too great a temptation to ignore — least of all, for scientists.
“It’s a just big waste of talent and wisdom to have people die in their 60s and
70s,” said Dr. Sinclair of Harvard.
One
for the Ages: A Prescription That May Extend Life,
NYT, 31.10.2006,
http://www.nytimes.com/2006/10/31/health/nutrition/31agin.html
Limbaugh says
actor Fox exaggerating his
disease
as stem cell issue churns
Updated 10/25/2006 8:58 AM ET
USA Today
By Andrea Stone
WASHINGTON — Rush Limbaugh has accused actor
Michael J. Fox of exaggerating the physical effects of his Parkinson's disease
in political ads urging viewers to vote for Democrats in next month's election.
The conservative radio host told listeners
Monday that Fox's lurching, palsied movements in a TV ad for Missouri Senate
challenger Claire McCaskill were "an act." Limbaugh noted that Fox, a longtime
advocate for research on embryonic stem cells, has said he sometimes does not
take his medication in order to illustrate Parkinson's severe physical effects.
Uncontrolled shaking and stiffness are among the symptoms of the nerve disease.
"If this was not an act," Limbaugh said later
on the show, "then I apologize."
John Rogers, Fox's spokesman, called Limbaugh's remarks "shameful."
It's an appalling, sad statement," Rogers said. "Anybody who understands
Parkinson's disease knows it's because of the medicine that one experiences"
body movements like those seen in the ad.
Fox, who has had Parkinson's for 15 years, is supporting candidates who would
vote to expand research using stem cells from human embryos.
Embryonic stem cells are the precursor cells to almost every tissue in the body.
Advocates of their use in research say they hold more potential to cure spinal
cord injuries, diabetes and other diseases than adult stem cells. Opponents say
the research with embryonic cells, which destroys the embryos, amounts to
abortion. This summer, President Bush used his first veto to kill a bill that
would have funded research using leftover fertility-clinic embryos that would
otherwise have been discarded.
Fox has also made ads for Senate candidate Ben Cardin in Maryland and Wisconsin
Gov. Jim Doyle.
In the McCaskill spot (claireonline.com), which aired during Game 1 of
baseball's World Series on Saturday, Fox says McCaskill, the state auditor,
"shares my hope for cures" while her opponent, Republican Sen. Jim Talent, wants
to "criminalize" expanded research.
Talent spokesman Rich Chrismer called the ad "false" and says Talent supports
"stem cell research that doesn't involve cloning or destroying a human embryo."
The Fox ads are part of a larger effort by Democrats who are using the issue as
another weapon against Republicans already hurting from an unpopular war in Iraq
and Bush's low approval ratings.
Democrats and interest groups are using ads, campaign events and celebrities in
at least 20 House, Senate and governor races to push for more federal funding
for embryonic stem cell research.
Fox's dramatic ads are "very effective" with suburban voters, seniors and
parents, says Evan Tracey of the non-partisan Campaign Media Analysis Group,
which tracks political advertising. "It puts the Republicans on the wrong side
of hope."
Other TV spots:
•Singer Sheryl Crow, a Missouri native and breast cancer survivor, appears in an
ad (www.missouricures.com) sponsored by the Missouri Coalition for Lifesaving
Cures, which backs a state ballot initiative to permit research on embryonic
stem cells.
•In Arizona, an ad (www .dccc.org/multimedia) sponsored by the Democratic
Congressional Campaign Committee features the granddaughter of Morris Udall, a
popular congressman who died of Parkinson's disease in 1998. Loren Udall, who
has the autoimmune disease lupus, says that "by voting in Congress to restrict
stem cell research, (Republican Rep.) J.D. Hayworth has played politics with
people's lives."
Brian Nick of the National Republican Senatorial Committee says such
"fear-mongering" ads distort the positions of candidates who favor research
using adult stem cells. "It's unfortunate they're using a good man like Michael
J. Fox as a political pawn to misrepresent people's view."
Sarah Chamberlain Resnick of the Republican Main Street Partnership, whose
members back embryonic stem cell research, says of Missouri's senator, "Talent's
entire race is going to come down to stem cells. (McCaskill has) been killing
him on it."
Limbaugh says actor Fox exaggerating his disease as stem cell issue churns, UT,
25.10.2006,
http://www.usatoday.com/news/politicselections/2006-10-24-limbaugh-fox_x.htm
Self-Portraits Chronicle
a Descent Into
Alzheimer’s
October 24, 2006
The New York Times
By DENISE GRADY
When he learned in 1995 that he had
Alzheimer’s disease, William Utermohlen, an American artist in London, responded
in characteristic fashion.
“From that moment on, he began to try to understand it by painting himself,”
said his wife, Patricia Utermohlen, a professor of art history.
Mr. Utermohlen’s self-portraits are being exhibited through Friday at the New
York Academy of Medicine in Manhattan, by the Alzheimer’s Association.
The paintings starkly reveal the artist’s descent into dementia, as his world
began to tilt, perspectives flattened and details melted away. His wife and his
doctors said he seemed aware at times that technical flaws had crept into his
work, but he could not figure out how to correct them.
“The spatial sense kept slipping, and I think he knew,” Professor Utermohlen
said. A psychoanalyst wrote that the paintings depicted sadness, anxiety,
resignation and feelings of feebleness and shame.
Dr. Bruce Miller, a neurologist at the University of California, San Francisco,
who studies artistic creativity in people with brain diseases, said some
patients could still produce powerful work.
“Alzheimer’s affects the right parietal lobe in particular, which is important
for visualizing something internally and then putting it onto a canvas,” Dr.
Miller said. “The art becomes more abstract, the images are blurrier and vague,
more surrealistic. Sometimes there’s use of beautiful, subtle color.”
Mr. Utermohlen, 73, is now in a nursing home. He no longer paints.
His work has been exhibited in several cities, and more shows are planned. The
interest in his paintings as a chronicle of illness is bittersweet, his wife
said, because it has outstripped the recognition he received even at the height
of his career.
“He’s always been an outsider,” she said. “He was never quite in the same time
slot with what was going on. Everybody was doing Abstract Expressionist, and
there he was, solemnly drawing the figure. It’s so strange to be known for
something you’re doing when you’re rather ill.”
Dr. Miller, Professor Utermohlen and others will lecture about art and
Alzheimer’s on Wednesday at 6 p.m. at the New York Academy of Medicine. For more
information: (212) 822-7272;
www.nyam.org/events .
Self-Portraits Chronicle a Descent Into Alzheimer’s, NYT, 24.10.2006,
http://www.nytimes.com/2006/10/24/health/24alzh.html
Troubled Children
Living With Love, Chaos and Haley
October 22, 2006
The New York Times
By PAM BELLUCK
PLYMOUTH, Mass. — When Haley Abaspour started
seeing things that were not there — bugs and mice crawling on her parents’ bed,
imaginary friends sitting next to her on the couch, dead people at a church that
housed her preschool — her parents were unsure what to think. After all, she was
a little girl.
“I thought for a long time, ‘She’s just gifted,’ ” said her father, Bejan
Abaspour. “ ‘This is good. Don’t worry about it.’ ”
But as Haley got older, things got worse. She developed tics — dolphin squeaks,
throat-clearing, clenching her face and body as if moving her bowels. She heard
voices, banging, cymbals in her head. She became anxiety-ridden over
run-of-the-mill things: ambulance sirens, train rides. Her mood switched
suddenly from excitedly chatty to inconsolably distraught.
“It’s like watching ‘The Sound of Music’ and ‘The Exorcist’ all at the same
time,” Mr. Abaspour said.
For her family, life with Haley, now 10, has been a turbulent stream of
symptoms, diagnoses, medications, unrealized expectations. Diagnosed as a
combination of bipolar disorder with psychotic features, obsessive-compulsive
disorder, generalized anxiety disorder and Tourette’s syndrome, her illness
dominates every moment, every relationship, every decision.
Haley’s fears, moods and obsessions seep into her family’s most pedestrian
routines — dinnertime, bedtime, getting ready for school. Excruciating worries
permeate her parents’ sleep; unanswerable questions end in frustrated hopes.
“The first time we took Haley to the hospital, I guess I expected that they
would put it all back together,” said her mother, Christine Abaspour. “But it’s
never all back together.”
At least six million American children have difficulties that are diagnosed as
serious mental disorders, according to government surveys — a number that has
tripled since the early 1990’s. Most are treated with psychiatric medications
and therapy. The children sometimes attend special schools.
But while these measures can help, they often do not help enough, and the
families of such children are left on their own to sort through a cacophony of
conflicting advice.
The illness, and sometimes the treatment, can strain marriages, jobs, finances.
Parents must monitor medications, navigate therapy sessions, arrange special
school services. Some families must switch neighborhoods or schools to escape
unhealthy situations or to find support and services. Some keep friends and
relatives away.
Parents can feel guilt, anger, helplessness. Siblings can feel neglected,
resentful or pressure to be problem-free themselves.
“It kind of ricochets to other family members,” said Dr. Robert L. Hendren,
president-elect of the American Academy of Child and Adolescent Psychiatry. “I
see so many parents who just hurt badly for their children and then, in a sense,
start hurting for themselves.”
Ms. Abaspour, 39, struggles to master the details of Haley’s illness, to answer
her obsessive questions, to keep her occupied. Mr. Abaspour, 50, who long
believed that “Haley was going to grow out of it,” has been gripped by anxious
thoughts and intrusive images that rattle him to tears on the hourlong commute
to his job as an anesthesia engineer at a Boston hospital. He imagines people
being crushed by trucks, someone hurting Haley, his own death.
Haley’s sister, Megan, 13, has been so focused on Haley and determined not to
add to her family’s burden that in June, after a quarrel with her parents, she
tied a T-shirt around her neck in a suicidal gesture.
“I feel like she gets all the problems and I feel like I have to take some of
that off of her,” Megan said. “It’s really difficult a lot to try to stay away
from babying her and helping her. I try to stay still but it just hurts, it
hurts inside.”
Haley, with her shy smile and obsidian eyes, is increasingly aware of her own
problems, although she cannot always express exactly what is going on inside.
“My mind says I need some help” is the way she explained it recently.
Her illness has caused great financial strain; although the Abaspours have
health insurance, they have been forced to draw on their savings and lean
heavily on their credit cards for living expenses. Still, they have bought a
trailer in a New Hampshire campground because there Haley finds occasional
solace, and relatives nearby understand the family’s ordeal.
The family wrestles with deciding whom to tell about Haley’s illness, and what
to say. Her worst symptoms are most visible at home and less apparent at the
public school and the state-financed therapeutic after-school program she
attends. Her parents say she works hard to hold herself together during the day
and then later, feeling more comfortable with her family, falls apart.
This disparity in behavior is not uncommon, said Dr. Joseph A. Jackson IV,
Haley’s psychiatrist, and “parents often get the brunt.”
Because of the contrast in Haley’s public and private behavior, her parents are
wary of telling people that she is mentally ill, as they might not notice.
“I don’t want anybody to pity her,” Mr. Abaspour said. But they also get
frustrated when teachers or relatives play down the seriousness of Haley’s
illness, or conclude that she is being manipulative or that another
child-rearing approach would help.
In the middle of last year, for example, a teacher did not understand Haley’s
need to leave the classroom to quiet the voices or relieve anxiety. Haley grew
so frustrated that she “would sit there in her chair and cry,” her father said.
The parents pressed school officials to switch her to another class.
“We’re sick and tired of trying to prove it to people,” Ms. Abaspour said.
Her husband added, “Everybody thinks they have the solution. When Joe Schmo
comes over for a drink, he says, ‘Try this, this will work.’ No, it won’t.”
Visions and Voices
From birth, it was clear that “I was dealing with something different,” Ms.
Abaspour said. Displaying a photo album with picture after picture of Megan all
smiles and Haley “crying, crying, crying,” she added, “We just thought we had a
very difficult child.”
Yet exactly what was wrong puzzled them for years, and even now, Ms. Abaspour
said, “Every day it’s something new, I swear.”
While increasing awareness of childhood mental illness has helped many children
and families, it can also create a misimpression that everything can be treated,
said Dr. Glen R. Elliott, chief psychiatrist at the Children’s Health Council, a
community mental health service in Palo Alto, Calif., and the author of
“Medicating Young Minds: How to Know if Psychiatric Drugs Will Help or Hurt Your
Child.” That can make families with complex cases feel “either genuine confusion
or pretend certainty,” Dr. Elliott said.
The Abaspours decided to speak with a reporter about Haley’s illness and its
impact on their family because they hoped it would help other families and make
society more hospitable for children like their daughter. Talking about it was
sometimes emotional, especially for Mr. Abaspour, whose eyes often clouded with
tears. But they also said they found it useful to articulate their feelings.
When Haley was 3 or 4, a pediatrician blamed tonsillitis-induced sleep apnea,
predicting that after her tonsils were removed, “ ‘you’ll see a totally
different child,’ ” Ms. Abaspour recalled.
“We thought, ‘This is what is wrong with our child. This is our answer,’ ” she
said. Preschool teachers suggested a learning disability. Later, Haley repeated
first grade. The Abaspours consulted therapists about the visions of friends in
the liner of the family’s pool and riding with Haley on her bike, and the voices
criticizing her or telling her to touch a certain table. When a neurologist
ruled out medical causes like Lyme disease, Ms. Abaspour recalled, her husband
said, “I think we should just give her a placebo — it’s all in her head.”
They got a cat, “though we weren’t cat people,” Ms. Abaspour said. Then they got
another because the first was “not the type of cat that Haley could throw over
her shoulder and squeeze.”
New symptoms kept emerging. For a while, when she was about 7, the voices “were
telling her she was a boy,” Ms. Abaspour said. “She had to constantly prove to
them that she wasn’t.”
Haley became obsessed with penises, which she called “bums.” She claimed to see
them though she was looking at fully clothed men and boys, her mother said.
“Then she felt guilty. She would come up to me and whisper, ‘I saw his bum, I
saw his bum.’ The bus driver or the little boy, anyone. It was constant.”
To halt the whispering, Ms. Abaspour suggested that they share a private signal:
Haley could flash a thumbs-up after a sighting. Haley also seemed preoccupied
with death, and on a highway would say that voices told her, “If that license
plate didn’t say such and such, she was going to die,” her mother said.
Once, Mr. Abaspour recalled, Haley “kept yelling that she wants to start over.”
The Treatment Puzzle
When she was almost 8, Haley visited Dr. Jackson at his office at the Cambridge
Health Alliance. He was struck by the results of a screening: Haley met full
criteria for virtually every mental disorder listed.
“Her symptoms,” he said, “suggested anxiety, morbid thoughts, obsessions
possibly of a sexual nature, frequent fluctuations in mood, periods of euphoria,
giddiness, irritability, rapid speech, auditory and visual hallucinations,
thought disorganization, vocal tics, distractibility, poor socialization in
school, sensory integration issues, attention impulse disorder, manic behavior,
sleep disturbance.”
Dr. Jackson wondered if the voices and the friends, which Haley told him were
“nowhere but everywhere,” were schizophrenic-like hallucinations or milder
thought distortions.
He also saw Haley’s mood swing from anxiety about a “disturbing dream in which
her mother was killed” to euphoria, as she gleefully drew a large, brightly
colored butterfly and a self-portrait with a too-big smile and a skirt that
ballooned as if she were floating. The pictures, he said, “scream” manic
sensibility, suggesting bipolar disorder.
Dr. Jackson prescribed an antipsychotic, Risperdal, one of a dozen drugs Haley
would try. Some helped initially, but the voices returned or side effects
developed.
Huge pills or bad-tasting liquid made Haley gag or throw fits.
“It was horrible, horrible, horrible,” her mother said, “and she’d pull us into
it because we had to make her take it.”
Lithium caused weight gain: clothes that fit her one day no longer did the next.
When Haley was 81/2, Mr. Abaspour said, “Let’s drop all of these medications and
see what happens.” He said, “I wanted to see her true self.”
The results chastened them. “You see her fine one day,” Mr. Abaspour said. “The
second day comes and she’s fine and you say, ‘You see, honey, there’s nothing
wrong with her.’ Then it’s the third day and she goes crazy and you feel like an
idiot.”
Haley resumed taking Risperdal. Then, abruptly, her condition worsened.
“She couldn’t function, she couldn’t go to school,” said Ms. Abaspour, who took
Haley to a hospital; she had to handle the crisis with her husband away in
London.
In the emergency room, Haley was manic and hyperarticulate, Ms. Abaspour
recalled. “I was a basket case.”
When Mr. Abaspour returned and saw Haley “like a zombie” in a hospital full of
out-of-control children, his first reaction was, “She can’t be in here.”
But the eight-day hospital stay made him grasp the severity of her illness.
“You look at an X-ray and you say it’s a fracture,” he said. “But this thing.
... Before then, there wasn’t solid evidence.”
A year later, school halls “would get scary because the voices would get
louder,” so Haley constantly visited the school’s nurse and psychologist, her
mother said. “She was going out of her mind.”
Haley was hospitalized again, and another antipsychotic drug, Abilify, muffled
the voices.
“I remember thinking, ‘Am I supposed to be happy about this?,’ ” Ms. Abaspour
said. She was grateful that something helped but distressed at the suggestion
that Haley was psychotic. The Abilify has not soothed Haley’s anxiety or stopped
her outbursts. And despite increases in the dosage, back are the voices (four
boys and a girl), the tics (eye squinting and hand clenching) and the “bums.”
Dr. Jackson, her psychiatrist, said Haley’s biggest asset was her “very caring
family” that was “seeking ways to shore themselves up” to better help her.
Ms. Abaspour said: “We ask ourselves sometimes, ‘Why? Why did it happen to us?’
Other times we see a child bald, going through chemotherapy. That’s the thing
about this — it’s on the inside, you can’t see it.”
Megan’s Heartache
I pretend no one is around me when my sister is there.
I feel a constant hurt inside.
I touch a rainbow of joyfulness in my mind when my sister and I are FINALLY
having a fun laugh together.
I worry that when one day I die, I won’t be there to help my sister.
I cry to the stars, pleading them to take me away from this madness at mind.
Megan’s sixth-grade writing assignment was to write a poem called “I Am.”
Virtually every line was about Haley.
Megan wrote of love, frustration, obligation, pain, embarrassment. Eighteen
months later, those feelings erupted.
Told to do dishes before calling a friend, Megan felt that the chore should be
Haley’s and stormed to her room. When her father said it was Megan’s
responsibility, “I really got mad and slammed the door,” she recalled. “He came
and ripped my phone right out of the wall.”
That was unusual for Mr. Abaspour, usually gentle or quietly humorous.
“I tried not to say something that would hurt her,” he said. “And definitely not
to touch her. So I took it out on the phone.”
Megan said her reaction was, “Why should I live?”
“I took a T-shirt and I put it around my neck,” she said. “Then I said, ‘No I
shouldn’t do this. I want to live but I don’t know another way out.’ ”
Siblings of mentally ill children often have such feelings, experts said.
Ten days of treatment helped Megan understand that “I felt pretty much like I
was another mom for Haley,” she said.
The Abaspours, who always gave Megan positive attention, were stunned. But Ms.
Abaspour said she might have unconsciously been relieved that Megan could get
Haley to laugh, or in other ways “take a little attention off me.”
For Megan, a doctor prescribed Prozac, but she became edgy and the suicidal
thoughts continued.
“When I’m doing dishes and I see a knife there, my mind’s like, ‘Pick up the
knife and kill yourself,’ ” Megan said. “I kind of just think, ‘Would things be
easier without me?’ ”
Now she has stopped taking medication and is seeing a psychiatrist. Her parents
are encouraging her to focus more on herself. She realizes, she said, “I’m
important.”
Still, trying not to help Haley is hard. “I don’t really feel the pain that she
feels,” Megan said, “but I feel that I should to make it even between us.”
Haley’s mother calls it “the ongoing search” — Haley’s obsessive quest for
novelty and for objects to hold or to stroke over her touch-sensitive skin.
“I need something to calm me down so I can learn how to end my frustration,”
Haley said. “I just get, like, sometimes, mad. I need to, like, hold it or hug
it or just play with it.”
She and her family search through stores, scavenge through her crawlspace
storage area and her bedroom full of Beanie Babies, toy cars, dolls. Megan said
she sometimes offered her own belongings for Haley, thinking, “if I get excited
about it she’ll decide it’s the right thing.”
But, Ms. Abaspour said, “she’s never satisfied.” Because her parents sometimes
brush the hair on her arm with a surgical brush from Mr. Abaspour’s hospital,
the family’s therapist recently suggested getting a soft lambskin.
Haley fixated on buying one, always asking as if it were a new thought: “Oh my
God, you know what just came to mind? If I get that animal fur...”
Megan found her a faux shearling vest to stroke instead, but Haley exploded.
“I wanted Megan to find something like that animal fur,” she wailed, convulsing
and weeping.
Anguished as he watched her, Mr. Abaspour said: “This is the point of no return.
She’ll scream and cry and kick. If the neighbors could hear, they would think we
were abusing the kid.”
Haley refuses to be consoled or touched, all the while saying, “Please help me,
please make it stop, please make it go away,” her mother said. The Abaspours
look on helplessly or send her to another room.
Haley’s eruptions, often 20 minutes long, occur almost daily, especially in the
evenings. They often begin with Haley revved up.
Before the lambskin incident, for example, she marched around, chatting giddily
about camp: “Today, today, today, we, um, instead of two periods of the game
thingies, they call it sessions, periods, each session or whatever, we went to
the picnic tables and we all went to the picnic tables and it was really fun.”
Haley’s parents struggled to track her unspooling sentences and scrambled
thoughts.
“Did you follow the bouncing ball?” Ms. Abaspour asked her husband, who replied,
“I don’t even see the ball, honey.”
Haley sighs, frowns and fidgets, eyes drooping before she falls apart. Sometimes
she hyperventilates or crawls under a table. It always ends with crying, but
sometimes she will start to laugh through her tears, becoming “all chipper
again, like manic,” Mr. Abaspour said.
Adds Ms. Abaspour: Later, “she says, ‘I’m sorry, I’m sorry,’ apologizing for who
she is.” Her father said: “It’s not like a hurt that you can kiss better. It
comes from within, and she doesn’t know why, and you can’t do anything about
it.”
A Mother’s Stoicism
Christine Abaspour, the youngest of four girls raised by a divorced mother, knew
what she wanted early in life. At 19, she left Massachusetts, joined a sister in
Florida and became a waitress. At 25, she met her husband-to-be, who was 11
years older. She was engaged in two weeks, married in nine months and a mother a
year later.
“We both wanted to have children right away, like you wouldn’t believe,” she
recalled.
Ms. Abaspour said that she had no regrets, and that Haley “was given to us for
some reason, and I keep waiting for the day when I realize why.”
Still, the experience has tested her stamina, and she avoids capitulating to
Haley’s whims and outbursts by imposing structure, consistency, even distance.
“I’m her mother,” Ms. Abaspour said. “I try to make it a better world for her, a
more comfortable world. I stay very strong for her and very encouraging for her.
If she comes out of a meltdown, I’ll say, ‘I knew that you could.’ I don’t make
her feel totally hopeless. It doesn’t give me any satisfaction, though, because
I still feel helpless. Unfortunately it just bites you in the face all day
long.”
Ms. Abaspour’s stoic approach, which her husband appreciates but cannot always
emulate, is “a good coping skill for parents,” Dr. Elliott, of the Children’s
Health Council, said. “It’s what happens to a family system when you’ve got a
source of chaos in the middle of it.”
After getting Haley ready for school, Ms. Abaspour feels she has already lived
an entire day. In the afternoon, “Haley walks in the door and I just want to
hold her and give her a big kiss like most kids,” Ms. Abaspour said. “Instead I
get a frown and tears and ‘Ooh, I had such a stressful day.’ ”
She said that every evening, a distraught Haley will “say to me her same 12
questions: ‘What’s going to happen when I need to go to school and I can’t leave
the classroom?’ or ‘What do I have to look forward to today?’ ”
By bedtime, Ms. Abaspour said, “your heart’s just breaking.”
To slake Haley’s thirst for “something to do,” Ms. Abaspour keeps her involved
in activities outside of school. Otherwise, the family ends up stopping for ice
cream or concocting other outings, because unstructured time allows Haley to
focus on the voices and anxiety. “Staying home is not an option,” Ms. Abaspour
said. “Honestly I could not keep her busy. Sometimes being around here on a
Saturday or Sunday, it’s almost toxic. She has multiple episodes — it’s like
living hell.”
Haley’s fears of noises, crowded streets and surprises force the Abaspours to
forgo amusement parks, apple picking or other traditional family activities.
When relatives visit “and you think it’s going to be relaxing and we’ll watch
movies and eat popcorn — that doesn’t happen in this family,” Ms. Abaspour said.
Instead, there are mood cycles, as when Haley marched around announcing, “I’m
going to make a really great art project,” then fell apart, wailing, “I don’t
know what to do.”
Ms. Abaspour stays unflustered. When Haley bawled, “I don’t have any markers,”
her mother replied, “Oh, don’t tell me you don’t have.”
But she found Haley a T-shirt to cut up and draw on, saying, “If I can get her
to do that kind of chop, chop, chop, mark, mark, mark, it kind of brings her
back.”
Ms. Abaspour said she had watched “everyone else in the family rush over to her,
and I won’t become a part of that. I make her be responsible for her own
feelings because I can’t be responsible for those. You still have to be a
regular parent. Honestly, she has to learn to soothe herself.”
But Ms. Abaspour doggedly monitors Haley’s progress. This summer, she visited
Haley at day camp and was dismayed that the child frequently declined to
participate, asking for the nurse.
Sitting out the swim period one day, Haley, wearing a “Keep It Cool” T-shirt,
listed her feelings on a worksheet: “stressed, axxouis, sick, shacky.”
At lunch, she mostly licked salt off pretzels. Asked to choose a word-card
matching her emotions, she picked “overwhelmed.”
Ms. Abaspour worries that as Haley becomes a teenager, her poor social skills
might get her “mixed up with the wrong kids” or lead her to use illegal drugs.
So she arranges play dates, but if friends are unavailable “it’s the end of the
world,” she said. If they are available, she said, Haley anxiously asks, “What
do I say, Mommy?”
Ms. Abaspour was recently laid off from a medical assistant’s job. Her former
co-workers understood her need to interrupt work to deal with Haley’s needs, she
said, and “didn’t look at me and say, ‘Her child’s crazy.’ ” Now she fears she
will not find an employer who is as tolerant, though the family needs the
income. Haley’s illness, the Abaspours were dismayed to discover, does not
qualify for disability assistance.
In August, Ms. Abaspour arranged an elaborate 50th-birthday surprise party for
her husband. They were “not always on the same page” about Haley at first, she
said, but their strong marriage helps her handle the strain.
So do bright spots, she said, like the day Haley “really kissed me.”
Still, she can get overwhelmed.
Sometimes she bolts awake at night, but she declines medication.
“I can’t climb in a shell and stay there forever,” she said, “although it seems
like some days where I’d want to be.”
A Father’s Anxiety
As a young man, Bejan Abaspour worried, especially about family.
Twenty years ago, for example, when his sister’s son was born, “I pictured my
nephew getting Super Glue in his eyes and I was calling my sister saying, ‘Make
sure you keep Super Glue away from him.’ ”
But the worries were not that intense — until Haley’s illness. After that, the
intrusive thoughts and images got worse, horrific scenes in which he imagines
himself as bystander or thwarted rescuer. “I’ll be driving next to a semi
tractor-trailer truck and all of a sudden I will picture someone getting crushed
by the wheel,” he said. “It’s usually an older lady or a kid. You get them out
from under the truck, but it doesn’t stop. I’m in the emergency room, trying to
help. I’m at the funeral. Then very easily, the tears come.”
Mr. Abaspour said he sometimes pictured Haley “getting lost somewhere, or
someone’s going to hurt her. I’m involved and trying to get the guy who did it
to stop. Sometimes I kill him. Sometimes it doesn’t get that far.”
Other times, he said, he imagines his death, seeing his family “at the funeral
home and I’m laying there. I try to see what’s going on at home, how Meggie’s
reacting to my death, how Haley’s reacting, what Christine is going through.”
He rehashes things Haley has said, like wanting to “start over” or her question:
“When I get really old, can I come back home? Will you be there?”
He wonders if his worrying laid genetic groundwork for Haley’s illness, “if I’m
the cause of what Haley’s going through.”
Until recently, Mr. Abaspour, who also has trouble sleeping, told no one about
his agonizing thoughts, not even his wife.
“I didn’t want to burden her,” he said. “I can handle it. So what if I’m driving
to work and I cry? So what if I only sleep for four hours?”
But last spring, the family’s therapist noticed “I had certain problems,” he
recalled. She encouraged him to tell his wife whenever he had disturbing
thoughts. Mr. Abaspour said he hoped that confronting his own anxiety would help
“get to the bottom of what Haley’s going through.”
He added, “It doesn’t matter for me, but for Haley.”
Families once kept illnesses like Haley’s quiet, afraid of being shunned or
disparaged.
Public acceptance has grown, but some misperceptions and prejudice remain, and
families feel conflicted: they want people to understand so the child can get
appropriate help, but they also fear that Haley will be mocked or ostracized.
“If they keep it a secret then they’re bad parents,” Dr. Elliott said. “If they
start spewing diagnoses, they’re subject to criticism because they’re not taking
responsibility, just laying it on the illness. Or they’re social pariahs because
there are some people who think that mental illness is contagious.”
Like other families, the Abaspours sometimes hesitate to publicly label their
daughter mentally ill. But they also want people to know, and they get
frustrated if people do not fully accept or understand it, or see her symptoms
“as a manipulative thing, or they feel like they can fix it themselves, maybe by
distracting her,” Ms. Abaspour said.
Her own family now understands and is very supportive, but it took some
convincing, she said.
“My mother would say, ‘She’ll be fine, she’ll be fine, there’s nothing wrong
with her,’ ” Ms. Abaspour said. “My sister says, ‘Well, she didn’t act like that
when she was over here.’ ”
Mr. Abaspour has not told most of his family, who live in England, because they
might worry excessively or not understand.
He told his sister, but “she was like I was when I first encountered the
situation — disbelief or denial,” he said. His sister, he said, has not told her
husband or her 20-year-old son, which created an odd atmosphere when they
visited the Abaspours in August. “When Haley did have one of her little
episodes, they were all like, ‘oh, oh,’ and they wondered why we weren’t running
over to her,” Ms. Abaspour said. “I would like to talk to them more about it. If
she had diabetes, they’d know she had diabetes.”
When, after reading a book for children with bipolar disorder, Haley said, “I
can’t wait to go to school and tell everybody I’m bipolar,” the Abaspours were
torn.
They discouraged her from announcing the diagnosis. But Haley did tell her
classmates, “ ‘I have a lot of noise going on in my head and sometimes I feel
anxious and sometimes I have to take a walk.’ ”
Some day, the Abaspours hope, Haley will have more effective drugs and better
coping skills, and society will be more tolerant, so she can lead an independent
life. But they have no illusions.
“This is not going away,” Ms. Abaspour said. Not for Haley or her family. “The
overflow of what Haley has is what has made all of us what we are today.”
Living With Love, Chaos and Haley, NYT, 22.10.2006,
http://www.nytimes.com/2006/10/22/health/22kids.html
Debate surrounds
end-of-life health care
costs
Updated 10/19/2006 3:55 AM ET
USA Today
By Julie Appleby
If you are dying in Miami, the last six months
of your life might well look like this: You'll see doctors, mostly specialists,
46 times; spend more than six days in an intensive care unit and stand a 27%
chance of dying in a hospital ICU. The tab for your doctor and hospital care
will run just over $23,000.
But spend those last six months in Portland,
Ore., and you'll go to the doctor 18 times, half of those visits with your
primary care doctor, spend one day in intensive care and stand a 13% chance of
dying in an ICU. You'll likely die at home, with the support of a hospice
program. Total tab: slightly more than $14,000.
Researchers at the Dartmouth Atlas Project, a program at the Dartmouth Medical
School that evaluates variation in medical care, analyzed Medicare data on
patients with chronic illnesses to develop those statistics, showing that it
costs far more to die in some parts of the country than in others.
While researchers are able to show differences
in costs, the real question remains how much of those additional
hospitalizations, tests and doctor visits resulted in better care or better
quality of life? Finding answers to that question is difficult and
controversial, but health policy experts say doing so will become increasingly
important as the U.S. seeks ways to slow the rapid rise in health care spending.
"There's a tremendous opportunity for both improving quality and enhancing
efficiency in the care of people with very serious illnesses at the end of
life," says geriatrician Joanne Lynn, who spent much of her career at think tank
RAND studying end-of-life care.
She says substantial progress could be made in slowing rising costs if the U.S.
health system could find better ways to reduce hospitalizations for people at
the end of life, such as providing more in-home services.
Portland and Miami reflect that tremendous variation among regions. The most
expensive city out of 309 hospital referral regions is Manhattan, at a cost of
$35,838 for the last six months; the least expensive is Wichita Falls, Texas, at
$10,913.
Estimates show that about 27% of Medicare's annual $327 billion budget goes to
care for patients in their final year of life.
While that's not altogether surprising given Medicare's demographics — most
patients are over 65 — researchers say it's important to find out if that is
money well spent.
While not the major factor driving health care spending, costs involved in
sustaining patients in their final days are likely to get a closer look by both
Medicare and private insurers as health costs continue to spiral and the
population ages.
Why costs vary
Why is it more expensive to die in some areas of the country than others?
The number of doctors and hospital beds is part of it: The more there are, the
more care a person gets. Also playing roles: the expectations of patients and
the practice patterns of doctors.
Portland has fewer ICU beds and specialists per person than Miami, which is also
more multicultural, with a greater variety of views on end-of-life medical care.
But experts on the end-of-life care say one main reason for the vast difference
between the two cities may be that in Oregon, doctors, or staff at hospitals and
hospices, encourage patients with life-threatening illnesses to talk about the
end of life, what kind of medical care they want and where they want to die. The
state has a history of such debate: Oregon residents have long supported
palliative care, a term usually used to describe medical care for the terminally
ill that focuses more on comfort treatments than cures. And, in 1994, voters
there became the first in the nation to approve doctor-assisted suicide, a
referendum signed into law in 1998.
"We have fewer hospitals and ICU beds than Miami does and, yes, that's a factor.
But making a plan and how everyone supports you to have that plan is what makes
the difference," says Susan Tolle, a medical doctor and director of the Center
for Ethics in Health Care at Oregon Health & Science University.
The ways people die in Portland and Miami illustrate the vast variation in what
is done at the end of life in America.
Across the nation, some patients spend much of their final weeks seeing
specialists, having tests, trying new drugs. Many die attached to machines, such
as ventilators, in hospitals.
For some patients, that's exactly the right care. Doing everything that can be
done to save an 18-year-old motorcycle-crash victim makes sense. But what about
an 85-year-old with heart failure, diabetes and cancer? Do you continue
aggressive chemotherapy?
Then the answers are not so clear-cut.
Complicating matters is that medicine often doesn't know what the most effective
treatments are. And doctors are trained to save lives. As a result, some
patients may be pushed into more than they want by a medical system that values
doing something over doing nothing, even when futile.
"One of the things that frustrates us all is to see care being provided in an
absolutely futile situation ... and doctors and hospitals are not accountable
but are also being rewarded (financially) for that (futile care)," says John
Santa, medical director for the Center for Evidence-Based Policy in Portland.
When not to treat
Not so long ago, Americans were felled by a bad infection or an accident or a
sudden illness, such as a heart attack. Advances in medicine mean more of us are
living longer, but often with disabilities.
"Many more of us make it to older age, and so there's much more we can do
(medically)," says geriatrician Lynn.
But, increasingly, ethicists, economists and patient advocates are questioning
whether the spending mentality is best for elderly patients or the long-term
financial future of programs such as Medicare.
"We are going to double the number of people who are sick, old and frail in
about 15 years," says Lynn. "It would be a good thing to try on some ways of
thinking about how to live that well ... and at a cost the community can
sustain."
She and others say there's not enough money to give everyone a treatment with a
one-in-a-million chance of success. "None of us wants to bankrupt our community
on desperate, long-shot treatments," Lynn says. "The question is, how do we
build a sustainable health system?"
Those questions about what care to give and when to quit are deeply personal. A
USA TODAY/Kaiser/ABC poll of 1,201 Americans taken by telephone in September
found the public divided on the answers.
When asked if it is better to keep a terminally ill person alive as long as
possible, regardless of the expense, or to make a judgment as to whether it's
worth the expense, 48% said it's better to weigh the costs, compared with 40%
who said to keep the person alive as long as possible, regardless of the cost.
Among those 65 and older, 60% said expense should be considered, compared with
28% who said cost should not enter the decision. The nationally representative
poll has a margin of error of plus or minus 3 percentage points.
Improving quality of care
Still, not everyone agrees that slowing spending at the end of life is a panacea
for rapidly rising health costs. Such costs are driven by a host of factors, of
which the amount spent in the last six months of life is but a part. "There are
so many things that would result in very substantial resources being saved, and
(end-of-life care), on my list of things, is not at the top," says Santa.
Things closer to the top of his list include unnecessary back surgeries,
hysterectomies and what he calls an over-reliance on some expensive brand-name
drugs when generics would work just as well.
But Santa and other proponents of the Oregon model say its importance goes well
beyond any cost savings that might result. Rather, they say it's a way to give
patients more control over their own medical treatment and is changing a culture
of medicine that has been reluctant to discuss dying.
Oregon's program allowing people to register their wishes on the single page
Physician Order for Life Sustaining Treatments (POLST) form began in 1995 and is
widely accepted in the medical community, although it took time to build.
On the forms, patients can say whether they want cardiopulmonary resuscitation,
antibiotics or feeding tubes. Conversely, they can specify that they want full
treatment, including breathing machines and feeding tubes. And for how long.
The forms differ from so-called advance directives, which are also called living
wills, which name someone to speak on behalf of a patient and state patient
wishes. Instead, the forms are doctor's orders, similar to directions written
into medical charts, that are recognized and followed by medical personnel from
technicians on ambulances to staff at hospitals and nursing homes.
Tolle says most of her patients want to talk about their care and the way they
want to die, although the adult children of many are often more reticent.
"It's actually not that difficult to talk to approximately 80% of my patients
for the first time about an advance plan," Tolle says. "What is horribly
difficult is to talk to their children, who are not ready to talk about Mom and
Dad dying."
She says younger people or those without life-threatening illnesses are
encouraged to fill out legal documents for an advance directive, mainly to name
a person who can make medical decisions for them if they are unable to make them
for themselves.
The POLST forms in Oregon, which are printed on bright pink paper and can be
transmitted electronically by hospitals and other medical providers, are "for
the individual who is in life's last chapter," she says.
Robert Smith, a 79-year-old retired accountant in Portland, says he brought up
the subject with his doctor and filled out the form as part of his overall
estate planning, which includes a will, a designation of someone to speak for
him if he is unable and funeral arrangements.
His form says he wants antibiotic treatment but does not want to be kept alive
artificially. "If there's no hope of my continuing to live, I do not want a
feeding tube," says Smith, who encourages others to write down their desires and
talk with family and friends about them. "It's part of the care you have for
your family, that you told them what to do," says Smith.
Tolle says the program's designers did not focus on whether it would save money.
"A few individuals might want to spend more and want everything done," says
Tolle. "And we would fight for them, too."
Debate surrounds end-of-life health care costs, UT, 19.10.2006,
http://www.usatoday.com/money/industries/health/2006-10-18-end-of-life-costs_x.htm
Fort Collins Journal
Seeking Modern Refuge
From Modern Life
October 19, 2006
The New York Times
By MINDY SINK
FORT COLLINS, Colo. — Every time her neighbors
treat their lawns with standard chemical herbicides, Caryl Schonbrun fears for
her life.
Ms. Schonbrun, 52, has multiple chemical sensitivity syndrome, which she says
leaves her vulnerable to whiffs of substances that her system can no longer
tolerate. She said that she was sensitive to ingredients in herbicides as well
as pesticides, and that exposure to the chemicals could put her body into
anaphylactic shock.
“It’s an illness that you have to depend on the kindness of neighbors and
friends and hope for the best,” she said.
But Ms. Schonbrun said she had found that was not enough and turned to lobbying
the City Council, the mayor, the neighborhood mediator and anyone else she
thought might be able to help.
Her goal was to get neighbors either to refrain from using such chemicals or to
notify her before applying them.
Her condition and her campaign have left local officials and neighbors grappling
with just how much responsibility they all have in coping with one woman’s
ailment.
“It’s a pretty complicated situation,” said Diggs Brown, a Fort Collins
councilman who has met with Ms. Schonbrun. “How do you balance the rights of one
neighbor who is using legal chemicals on their lawn on private property and
somebody who apparently has a chemical sensitivity?”
Just the mention of chemical sensitivity can be controversial, as there remains
widespread doubt in the general medical community about whether it is a real
diagnosis. Even the term “multiple chemical sensitivity syndrome” is polarizing
in the medical and environmental health communities. Ms. Schonbrun said that she
had been classified as “disabled with chemical injury” and that she received
disability checks.
“The bottom line is that the condition is very much in dispute,” said Dr. Edward
B. Holmes, director of the Occupational and Environmental Health Clinic at the
University of Utah. “There seems to be, in my experience, a significant number
of people that have this kind of conglomeration of symptoms that fit into a
pattern strongly with psychiatric conditions.”
Dr. Holmes said that in rare cases someone might have a true allergy to a
specific chemical.
On the other side of the debate are specialists like Dr. Claudia S. Miller,
professor of environmental medicine at the University of Texas Health Science
Center at San Antonio, who said practitioners were hearing about more cases of
chemical sensitivities.
“There is no reliable prevalence data because the illness presents in such
varied ways,” Dr. Miller said in an e-mail message. “But estimates of the number
of persons who report having multiple intolerances that they recognize and that
cause them to rearrange their lives ranges from 3 to 6 percent of the
population.”
Dr. Miller said chemical sensitivities or intolerances could be caused by a
specific exposure to a toxic substance or by a number of exposures. There is no
known cure.
Often, people with severe chemical sensitivities remove themselves from urban
areas completely, but Ms. Schonbrun said she could not face such isolation and
did not want to be too far from her family or health care facilities.
After her diagnosis six years ago, Ms. Schonbrun left her job as a nurse in San
Diego and moved with her husband, Bob, to Tucson, where they stayed for a year.
When she became even sicker, the couple moved to Fort Collins, a college town of
about 130,000 with strong agrarian roots, to build a “safe” house with features
that include an elaborate venting system and a tar-free roof to allow her to
live as free of offending chemicals as possible.
Ms. Schonbrun has added her name to the Colorado Department of Agriculture’s
registry of pesticide-sensitive people so she will be notified and can stay
indoors when there is any commercial spraying.
Some people question the Schonbruns’ choice to relocate to their tidy and
rapidly expanding subdivision with farms and ranches close by.
“With a condition like that, they choose to move into a residential area,” said
Curt Richards, who lives across the street from the Schonbruns and said that the
dispute had escalated to the point that he had obtained a restraining order
against Mr. Schonbrun. “The bottom line is, we’re not breaking any laws. We have
modified how we take care of our property that requires more of my time and
money, but that’s not good enough.”
Ms. Schonbrun said she had twice had to call for an ambulance when her neighbors
used herbicides she could not tolerate.
The Schonbruns bought the first batch of nontoxic herbicides for some neighbors,
including Mike Cada, who lives next door.
“I’m willing to do it as long as it’s effective,” Mr. Cada said, noting that the
nontoxic mixture cost at least 40 percent more than traditional herbicides.
No local ordinances require private citizens to notify neighbors when they apply
pesticides. According to the National Conference of State Legislatures, six
states have laws that address overspraying and improper use of pesticides around
humans(especially children); two others are considering such laws.
“It’s been said that people with this condition are the new homeless,” Ms.
Schonbrun said. “We were lucky enough to build a nontoxic home, but it’s still a
never-ending struggle to live in a safe all-around environment.”
Seeking Modern Refuge From Modern Life, NYT, 19.10.2006,
http://www.nytimes.com/2006/10/19/us/19chemical.html
Geriatrics Lags
in Age of High-Tech
Medicine
October 18, 2006
The New York Times
By JANE GROSS
Margaret Mary Foley, 97, just wasn’t herself.
Overnight, she stopped eating, went from mildly confused to disoriented, and was
unable to urinate. When her panicked family rushed her to the emergency room,
doctors did invasive tests, difficult for a woman her age, and then suggested
surgery.
But when Mrs. Foley saw a geriatrician at Mount Sinai Medical Center, surgery
proved unnecessary. The geriatrician, Dr. Rosanne M. Leipzig, suspected a silent
infection — something the other doctors had missed because Mrs. Foley had no
fever, as old people rarely do.
Indeed, within days, antibiotics had done the trick. For the Foley family, it
was a welcome result. They had reason to count themselves fortunate to have
found a doctor who specialized in treating the elderly.
Even as the population ages and more people like Mrs. Foley need them,
geriatricians are in short supply. It is a specialty of little interest to
medical students because geriatricians are paid relatively poorly and are not
considered superstars in an era of high-tech medicine. In fact, the credo of
geriatric medicine is “less is more.”
In 2005, there was one geriatrician for every 5,000 Americans 65 and older, a
ratio that experts say is sure to worsen. Of 145 medical schools in the United
States, only 9 have departments of geriatrics. Few schools require geriatric
courses. And teaching hospitals graduate internists with as little as six hours
of geriatric training.
The mismatch between supply and demand is “a troubling issue for us,” said Dr.
Leo M. Cooney, a professor at Yale University School of Medicine. In a good
year, Dr. Cooney said, one of 45 internal medicine residents decides to be a
geriatrician.
The rest, he said, choose “super specialties” like cardiology or oncology. This,
despite the fact that geriatricians reported the highest job satisfaction of any
specialty in a 2002 survey in the journal Archives of Internal Medicine.
Interest is also low at the University of Oklahoma College of Medicine, which
has a rare requirement that medical students do a four-week rotation in
geriatrics. Eighty percent said it was time well spent, but less than 10 percent
considered it as a career, said Dr. Marie A. Bernard, chairwoman of the
geriatrics department. “They want to do laser-guided this and endoscopic that,”
Dr. Bernard said.
Caring for frail older people is about managing, not curing, a collection of
overlapping chronic conditions, like osteoporosis, diabetes and dementia. It is
about balancing the risks and benefits of multiple medications, which often
cause more problems than they solve. And it is about trying nonmedical
solutions, like timed trips to the bathroom to improve bladder control.
But these are common-sense remedies in a health care system that rewards the
heroics of specialists, in both compensation and prestige. The best-paid doctors
are those who do the most procedures; radiologists and orthopedic surgeons top
the list with average annual incomes of $400,000. Geriatricians, who do a
residency in internal or family medicine and then a fellowship in geriatrics,
are near the bottom, at $150,000 a year.
While fellow residents followed the money, Dr. Amit Shah, who had the luxury of
no medical school debt, chose a geriatrics fellowship at Johns Hopkins
University, despite being dissuaded by many people.
The most memorable discouragement came during his residency, from a
pulmonologist, Dr. Shah said.
“When I passed him in the hall, he would shake his head and mutter, ‘Waste of a
mind,’ ” he said. “My retort was always that the geriatric population is often
the most complicated, not only medically but also socially and psychologically,
and that was exactly the specialization you should want your top students going
into.”
Reimbursement drives doctors’ compensation. Gastroenterology, for instance,
became more lucrative — and popular — once Medicare, which sets the standard for
most other health insurance, began paying for screening colonoscopies.
Geriatricians joke that they are waiting for the invention of a geriscope, so
that they too can bill for procedures.
Meanwhile, much of what they do — communicating with family members,
discouraging unnecessary tests — is time consuming but not reimbursed.
Another disincentive is the lowly status of geriatrics at most of America’s
medical schools, which expect more ambitious choices from top residents like Dr.
Shah. In Britain, where every medical school has a geriatrics department, it is
the third most popular specialty. Reimbursement there goes up with the age of
each patient, a formula that improves compensation.
Historically, the explanation for not requiring geriatric training in this
country has been that a majority of hospital patients are old, and thus
doctors-in-training absorb what they need to know by osmosis. Nonsense, said Dr.
Robert N. Butler, president of the International Longevity Center in New York
and the first chairman of geriatrics at Mount Sinai. “All patients have hearts,”
Dr. Butler said, “but that doesn’t make all doctors cardiologists.”
One proposed solution to the shortage is for geriatricians to limit their
practice to the frailest of the elderly, generally those past 85, along with a
subset in the 65-to-85 age bracket who have complicated needs. According to a
2002 study at Johns Hopkins University, 20 percent of those 65 and older have at
least five chronic conditions.
Another solution, gaining a foothold among the nation’s top academic
geriatricians, is to focus on teaching the core principles of their specialty to
everyone, be they surgeons or discharge planners, because it is unrealistic to
assume there will be enough geriatricians to go around.
“If we got to the point where everybody in the health care system was an expert
in caring for older people, we wouldn’t need geriatricians,” said Dr. Cooney of
Yale. “Or we wouldn’t need them as frontline providers. We’d be like
consultants, making sure everyone else was as skilled as possible.”
Specialists, internists and emergency room doctors without sufficient training
in geriatrics can pinpoint their own inadequacies. In recent surveys by The
Journal of the American Medical Association, many said they were unprepared to
deal with end-of-life decisions, communication with family caretakers,
depression and other issues of aging.
That lack of training can lead to misdiagnosis, because it is often tricky to
tell the difference between physical, psychological and cognitive conditions in
this age group. That was the case for Rita Zaprutskiy, 75, of Houston who went
to the emergency room with a painful arthritic knee, had surgery, was given an
array of pain medications and then seemed to lose her mind.
Four hospitalizations and six months later, Mrs. Zaprutskiy’s daughter said, the
family was urged to put her in a nursing home because of severe dementia.
Instead, her daughter, Yelena Schwarz, tried one last psychological evaluation,
at a county hospital, and unwittingly wound up in a geriatric unit. There the
doctors knew, from the sudden onset of her symptoms, that Mrs. Zaprutskiy did
not have dementia, but rather treatable psychiatric conditions, including
depression.
One way to sharpen the skills of assorted specialists is to welcome them at
continuing education classes for geriatricians. At a popular Mount Sinai seminar
called “The Hazards of Hospitalization,” a nongeriatrician asked Dr. Helen M.
Fernandez how she would deal with a 90-year-old woman in the emergency room with
dizziness.
After hearing the woman’s history, Dr. Fernandez said she would fight against
admission. “You need to be brave enough to march down to the E.R.,” she said,
“and tell the attending she’s your patient and you want to peel her off some of
her meds before doing a full cardiac work-up.”
In another course, “The 10 Minute Geriatric Assessment,” Dr. Fredrick T. Sherman
told students to “get the focus off the stethoscope” and watch their patients
move around. Can a woman get out of a chair without pushing off with her hands?
That means she can still use the toilet. Can a man put on his socks? If not, he
will soon need someone to dress and bathe him.
“We want to know what they can do and what they can’t do,” Dr. Sherman said.
“That’s a better predictor of the future than a head-to-toe exam.”
A new form of geriatric training comes from elderly patients recruited as
mentors, like Alberta Harris, 85, who lunches with students at the University of
Oklahoma College of Medicine, regaling them with stories of her life. Residents
learn other lessons when they visit the elderly at home. Many doctors consider
family members impositions on their time. Seeing them as day-to-day caretakers
makes it clear that in geriatrics, an adult daughter, like Mrs. Zaprutskiy’s, is
an essential ally.
Ordinary floor nurses can also bring a geriatric sensibility to a hospital. An
institute at the New York University School of Nursing helps small community
hospitals identify nurses with an affinity for the elderly and provides them
with a training curriculum and guidance on how that nurse can be a resource to
others.
To increase the number of specialists, N.Y.U. and other nursing schools are
building a cadre of geriatric nurse practitioners. Many work in hospital units
reserved for the frailest patients, who can spiral downward quickly from a
setback like a skin infection or a broken rib.
Mrs. Zaprutskiy was treated in such a unit, run by Dr. Carmel Bitondo Dyer of
the Baylor College of Medicine. On a recent visit, while her daughter and doctor
discussed the case, Mrs. Zaprutskiy played Russian and Yiddish folk songs on a
piano in the day room, her crooked fingers moving gracefully across the
keyboard.
Ms. Schwarz wondered if her mother’s psychiatric condition had been caused by
medication. Dr. Dyer said there was no way of knowing for sure. But misdiagnosis
and overmedication of the elderly is common.
“We see it all the time — elderly people who go from hospital to hospital with
no results,” Dr. Dyer said.
“When patients are diagnosed correctly and care is managed accordingly, we see
great improvements,” she continued. “Sometimes we don’t cure them; we just make
them feel better. But that’s a good thing.”
Laura Griffin contributed reporting.
Geriatrics Lags in Age of High-Tech Medicine, NYT, 18.10.2006,
http://www.nytimes.com/2006/10/18/health/18aged.html
AIDS activist Jeff Getty dead at 49
Posted 10/15/2006 1:54 AM ET
AP
USA Today
JOSHUA TREE, Calif. (AP) — Jeff Getty, a
prominent AIDS activist who in 1995 received the first bone-marrow transplant
from a baboon to treat the disease, has died. He was 49.
Getty died Monday of heart failure, following
treatment for cancer and a long struggle with AIDS, at the High Desert Medical
Center in Joshua Tree, said Ken Klueh, his partner of 26 years.
Before antiviral drug combinations were used successfully by AIDS patients,
Getty grabbed national attention in December 1995 for becoming the first person
ever to receive a bone marrow cell transfusion from one species to another. His
transplant at San Francisco General Hospital used cells taken from a baboon,
with the hope that the primate's natural AIDS resistance would take root in his
own system.
The procedure, ultimately unsuccessful, sparked furious debate over the moral
and medical implications of cross-species transplants.
"That trial reflects the level of desperation at the time," said Dr. Steven
Deeks, the University of California, San Francisco, professor who was the
experiment's lead investigator. "Jeff was just hanging on to his life. He
inspired us that a risky and aggressive intervention was worth trying."
While the baboon bone marrow cells quickly disappeared from his system, Getty's
health seemed to dramatically improve. He went on help pave the way for the drug
cocktail HAART — or highly active anti-retroviral therapy — that routinely keeps
many HIV and AIDS patients alive today.
"He is emblematic of a whole group of men who survived AIDS in the early 1980s
and 1990s, and made it into the HAART era, but had developed so much resistance
to the drugs that they never got their virus fully under control," Deeks said.
Since being diagnosed with AIDS in the days when the disease still was known as
"the gay cancer," Getty was a fierce activist, volunteering to test experimental
drugs, getting thrown in jail for protesting against pharmaceutical companies
and even throwing a coffin on a hospital lawn to demand organ transplants for
patients.
"He was the bravest of the brave. He was committed to getting results, even
where it was clear that it wouldn't help him," said state Sen. Carole Migden,
who worked with Getty when she was an Assembly member.
A former University of California policy analyst, Getty had a keen intellect
that helped him navigate the science and politics of the disease, but he also
could be difficult and demanding, colleagues said.
"He wasn't easy to work with," said Michael Lauro, an organizer who teamed with
Getty in the advocacy groups Act Up Golden Gate and Survive AIDS. "That's how
people with great vision, great hearts, and great drive are like. He could get
things done."
Getty is survived by Klueh, his father and two sisters.
Plans for a memorial service were pending.
AIDS
activist Jeff Getty dead at 49, UT, 15.10.2006,
http://www.usatoday.com/news/nation/2006-10-15-obit-getty_x.htm
Tacit Silence on Stem Cell Research
in
Missouri Race
October 15, 2006
The New York Times
By SUSAN SAULNY
KIRKSVILLE, Mo. — Over cocktails one recent
Monday night at a Democratic fund-raiser in New York, Claire McCaskill, the
Democratic Senate candidate in Missouri, played up her support for stem cell
research.
But at a campaign appearance here in rural and largely conservative Kirksville,
Ms. McCaskill never mentioned the subject.
Similarly, her Republican opponent, Senator Jim Talent, came out against a
statewide ballot measure on stem cell research at the strong urging of
conservative Christians. But when Mr. Talent recently addressed an electricians’
trade group at a resort on the Lake of the Ozarks, he did not speak of his
opposition.
Just a few months ago, the Missouri stem cell research initiative on the
November ballot was a defining issue of the campaign, as both candidates tried
to firm up support among the party faithful in one of the tightest Senate races
in the country. But now, as Mr. Talent and Ms. McCaskill reach beyond their
traditional bases, the emotionally charged ballot measure — which would allow
the research and possibly provide state financing for it — is almost too hot to
touch.
In a race that appears to be a dead heat, the result has been an odd sort of
mutual quietness, where the opposing camps seem to agree that the less said on
the stump about stem cell research, the better.
“I’ve urged everyone to make those decisions on their own,” Mr. Talent said
after the speech to the electricians, in Osage Beach, Mo., when asked about the
ballot measure. “I’ve tried not to make it political.”
Ms. McCaskill denied shying from the issue but acknowledged it was not part of
her standard campaign speech.
“It’s not that I’m ignoring it, but the stem cell issue usually comes up in the
context of question and answer,” she said after a debate in Clayton, Mo. “People
are confused and want to talk about it.”
The truth of the matter, campaign analysts say, is that Mr. Talent and Ms.
McCaskill are battling over a tiny percentage of undecided voters and dare not
risk offending them by drawing attention to such a polarizing issue.
The race here is one of six nationwide in which Democrats see the possibility of
picking up a Republican seat to win control of the Senate; as such, there is
little margin for error for either party. Even in a recent national television
appearance on MSNBC, when the two candidates were asked about stem cell
research, Mr. Talent and Ms. McCaskill were measured in their responses, and
careful to use language that would not offend.
Robert Hunt Sprinkle, the editor in chief of Politics and the Life Sciences, a
journal edited at the University of Maryland, has tracked how the stem cell
research issue has figured in elections nationwide. Mr. Sprinkle said it was
“quite sensible” that the two candidates in Missouri had backed away from
“defending a view on a topic of arcane technological content” in a close
campaign.
“This is a debate that is entered at one’s peril in the campaign context, when a
sound bite is removed for analysis,” he said. “These are very treacherous
waters.”
The dynamic is markedly different in several other states, where Democratic
candidates have made stem cell research a bigger part of their campaigns, in
part because of evidence of broad public support for the research in those
states and because of the wedge it sometimes drives between far-right and
moderate Republicans.
In Wisconsin, the incumbent Democratic governor, James E. Doyle, has made his
steady support of all permissible forms of stem cell research almost a daily
mantra in his race against Representative Mark Green, a Republican who favors
setting stricter limits.
In the Maryland race for the Senate, Lt. Gov. Michael Steele, a Republican, is
running against Representative Benjamin L. Cardin, a Democrat who has tailored
his message to two main themes: the war in Iraq and his support for stem cell
research.
“Ben Cardin is doing what I expected Claire McCaskill to do, which is bring it
up,” said Trevor Parry-Giles, an associate professor of political communication
at the University of Maryland. “It might be one of those issues that plays
better on the coasts for Democrats, but Republicans face a tougher road on this
one because they need moderate independent voters.”
In Missouri, Mr. Talent has found himself tripping over the Republican divide.
Some more moderate Republicans, including Gov. Matt Blunt and John C. Danforth,
the former United States senator, are backing the stem cell research referendum,
while more conservative legislators, including Representative Todd Akin, are
speaking out against it, particularly to Christian congregations.
At first, Mr. Talent chose to steer clear of the issue, hesitating to take a
position on the ballot measure before relenting under pressure from Christian
conservatives. The senator had already angered many conservatives by removing
his name from a Senate bill opposed to cloning, so there was some
bridge-building to be done.
“This is a difficult issue,” Mr. Talent said in an interview. “It comes up a
fair amount, but I’ve been talking about my priorities and what they’re going to
be. Generally, I’ve focused on what I’ve done.”
And as of late, Ms. McCaskill has made that task easier for Mr. Talent by also
sidestepping the stem cell debate. Like many Democrats facing off against
incumbent Republicans, Ms. McCaskill, the Missouri state auditor, has
highlighted Mr. Talent’s close association with an unpopular White House and
pressed national issues like security, the war in Iraq, taxes and health care.
“He agrees with President Bush more than I agree with my husband,” Ms. McCaskill
said of Mr. Talent in an interview. “I think it’s very hard for Missourians to
accept that he’s an agent of change. In contrast, I have very independent
branding.”
The largest group in the state promoting stem cell research, the Missouri
Coalition for Lifesaving Cures, which is responsible for putting the initiative
on the ballot, has steered clear of questions about the Senate race because of
its nonpartisan stance.
The group’s chairman, Donn Rubin, said it was trying to pitch a large tent.
“Our initiative is supported by many denominations, Christian and other, who
believe in this research as a means to alleviate suffering,” Mr. Rubin said.
“Any one of us could be a patient tomorrow and we all have a stake in seeing
this amendment pass.”
If the measure were to pass — and polls indicate that a majority of Missourians
support it — Missouri would join California as the only states to include the
right to perform stem cell research in its state constitution. But unlike the
California measure, which designated billions of dollars for the research, the
Missouri amendment does not include a commitment to financing. (It does not bar
the possibility of it, however.)
The ballot measure would guarantee that any stem cell research that is legal
under federal law could be performed in Missouri. Mr. Rubin said the coalition
sought to get the issue on the ballot in direct response to efforts for years by
conservative lawmakers to ban the cloning procedure involved in some forms of
the research.
In the most controversial form of stem cell research, embryos are cloned and
their stem cells are removed. This practice has ignited the political debate
about whether life is being destroyed.
“This is the big one, this is the biggest pro-life issue voters have ever been
confronted with,” said Pam Fichter, the president of Missouri Right to Life.
“This is the people deciding whether they want to enshrine in the constitution
the right to clone and kill human embryos.”
Given the void in the discourse at the candidates’ level, many voters have been
left to sort through a barrage of advertisements financed by independent groups.
On billboards, on the radio and on television, the proposed amendment has been
dubbed the “kill bill” by anti-abortion groups and conservative Christians.
Advocates for the measure equate its passing with the guarantee of lifesaving
cures.
Meanwhile, the Senate candidates continue to look for swing voters. Ms.
McCaskill is working long hours to shore up her standing in the state’s rural
counties, where weak support from conservative voters contributed to her narrow
defeat in the governor’s race in 2004 and where opposition to the stem cell
initiative tends to be strong. At the same time, Mr. Talent is trying to win the
support of more liberal voters in urban areas, where his conservative views on
stem cell research generally are not well received.
“They’re raiding the traditional backyard of the other,” said Professor Lana
Stein, who heads the political science department at the University of Missouri,
St. Louis.
Tacit
Silence on Stem Cell Research in Missouri Race, NYT, 15.10.2006,
http://www.nytimes.com/2006/10/15/us/politics/15stem.html
Alzheimer’s Drugs Offer No Help,
Study
Finds
October 12, 2006
The New York Times
By BENEDICT CAREY
The drugs most commonly used to soothe
agitation and aggression in people with Alzheimer’s disease are no more
effective than placebos for most patients, and put them at risk of serious side
effects, including confusion, sleepiness and Parkinson’s disease-like symptoms,
researchers are reporting today.
The report, based on a large government comparison of the drugs’ effectiveness,
challenges current practice so sharply that it could quickly alter prescribing
habits, some experts said. About 4.5 million Americans suffer from the
progressive dementia of Alzheimer’s disease, and most patients with the advanced
disease exhibit agitation or delusions at some point.
The drugs tested in the study — Zyprexa from Eli Lilly; Seroquel from
AstraZeneca; and Risperdal from Janssen Pharmaceutical — belong to a class of
medications known as atypical antipsychotics. The drugs are used to treat
schizophrenia and other psychoses, and are commonly prescribed for elderly
patients in long-term care facilities.
About a third of the estimated 2.5 million Medicare beneficiaries in nursing
homes in the United States have taken the medications, researchers found. And
the use of atypical antipsychotics in the elderly accounts for an estimated $2
billion in the annual sales of the drugs, much of the cost paid by Medicare and
Medicaid.
Spokesmen for Lilly, AstraZeneca and Johnson & Johnson, which owns Janssen,
noted that the drugs were not approved by the Food and Drug Administration for
use in Alzheimer’s patients, and that the companies did not market them for that
purpose.
The results of the study, published today in The New England Journal of
Medicine, simply reflected the need for more research into the treatment of
behavioral problems in Alzheimer’s patients, the spokesmen said.
Prescribing information for the drugs warns that patients with
Alzheimer’s-related psychosis “are at increased risk of death compared to
placebo.”
But the medications are commonly prescribed for Alzheimer’s patients “off label”
by doctors because families are desperate, because these drugs sometimes seem to
help, and because company-sponsored doctors promoted them.
“The question is whether these drugs have a place in the treatment of
Alzheimer’s patients at all,” said Dr. Jason Karlawish, an associate professor
of medicine at the University of Pennsylvania who wrote an editorial
accompanying the study. “I think the answer is yes, but only for a subgroup of
patients who can tolerate them, and in facilities that have the expertise to
manage the side effects.”
In the study, researchers followed 421 Alzheimer’s patients with disabling
agitation, delusions or hallucinations who were randomly assigned to receive
either dummy pills or one of the three antipsychotic drugs. Doctors adjusted the
doses as needed, tracked how long they stayed on the drugs, and noted their
improvement, if any.
Experts say that the amount of time a patient spends on a medication is an
important measure of its usefulness, because patients often stop taking a drug
if it is not doing any good or if the side effects are intolerable.
After 12 weeks, “there were no significant differences between the groups with
regard to improvement” on a scale that measured symptom relief, said Dr. Lon S.
Schneider, professor of psychiatry, neurology and gerontology at the University
of Southern California School of Medicine, and the lead author of the study.
The researchers also found no significant difference in the amount of time the
patients stayed on the drugs or the placebos; about 80 percent stopped taking
the drugs and the placebos alike before the end of the study. But those on the
drugs were far more likely to quit because of side effects.
The side effects included sedation in 15 percent to 24 percent of the patients,
and confusion in 6 percent to 18 percent; both symptoms can increase the risk of
falls. And 12 percent of the patients on either Zyprexa or Risperdal experienced
Parkinson’s-like symptoms, including tremors.
“What the study does indicate is that this is a very sensitive population and
that any treatment needs to be done with a lot of forethought and constant
reevaluation” said Dr. Bruce J. Kinon, a Lilly psychiatrist.
Dr. Thomas R. Insel, director of the National Institute of Mental Health, which
financed the research, said, “What this study shows is that these drugs are
clearly not the answer; they may be helpful for a minority of patients but we
need to come up with better medications.”
Dr. Gary Kennedy, director of geriatric psychiatry at Montefiore Medical Center
in the Bronx, said that the results gave psychiatrists the first clear picture
of what many had observed in their practices: that improvement on the drugs is
usually modest at best, and that behavior and environment are often more
important in managing combative behaviors.
“Oftentimes the family is unwittingly provoking the agitation,” Dr. Kennedy
said.
A demented, confused person, he noted, can become suddenly aggressive over
seemingly trivial things, like a change in daily routine or feeling crowded or
rushed. “Working on these kinds of behavioral factors should always be the first
line of treatment,” Dr. Kennedy said.
The report is the third large study in the last year to conclude that atypical
antipsychotics are not as effective or as safe as initially portrayed. Last
year, government researchers found that three of four drugs tested were no more
effective than an older, far less expensive drug in treating schizophrenia — the
disorder for which the medications were originally approved.
And last week, English researchers published a study that found that
schizophrenia patients did as well on older medications — or better — than on
newer, atypical drugs.
Alzheimer’s Drugs Offer No Help, Study Finds, NYT, 12.10.2006,
http://www.nytimes.com/2006/10/12/health/12dementia.html
Out-of-Body Experience?
Your Brain Is to Blame
October 3, 2006
The New York Times
By SANDRA BLAKESLEE
They are eerie sensations, more common than one might
think: A man describes feeling a shadowy figure standing behind him, then
turning around to find no one there. A woman feels herself leaving her body and
floating in space, looking down on her corporeal self.
Such experiences are often attributed by those who have them to paranormal
forces.
But according to recent work by neuroscientists, they can be induced by
delivering mild electric current to specific spots in the brain. In one woman,
for example, a zap to a brain region called the angular gyrus resulted in a
sensation that she was hanging from the ceiling, looking down at her body. In
another woman, electrical current delivered to the angular gyrus produced an
uncanny feeling that someone was behind her, intent on interfering with her
actions.
The two women were being evaluated for epilepsy surgery at University Hospital
in Geneva, where doctors implanted dozens of electrodes into their brains to
pinpoint the abnormal tissue causing the seizures and to identify adjacent areas
involved in language, hearing or other essential functions that should be
avoided in the surgery. As each electrode was activated, stimulating a different
patch of brain tissue, the patient was asked to say what she was experiencing.
Dr. Olaf Blanke, a neurologist at the École Polytechnique Fédérale de Lausanne
in Switzerland who carried out the procedures, said that the women had normal
psychiatric histories and that they were stunned by the bizarre nature of their
experiences.
The Sept. 21 issue of Nature magazine includes an account by Dr. Blanke and his
colleagues of the woman who sensed a shadow person behind her. They described
the out-of-body experiences in the February 2004 issue of the journal Brain.
There is nothing mystical about these ghostly experiences, said Peter Brugger, a
neuroscientist at University Hospital in Zurich, who was not involved in the
experiments but is an expert on phantom limbs, the sensation of still feeling a
limb that has been amputated, and other mind-bending phenomena.
“The research shows that the self can be detached from the body and can live a
phantom existence on its own, as in an out-of-body experience, or it can be felt
outside of personal space, as in a sense of a presence,” Dr. Brugger said.
Scientists have gained new understanding of these odd bodily sensations as they
have learned more about how the brain works, Dr. Blanke said. For example,
researchers have discovered that some areas of the brain combine information
from several senses. Vision, hearing and touch are initially processed in the
primary sensory regions. But then they flow together, like tributaries into a
river, to create the wholeness of a person’s perceptions. A dog is visually
recognized far more quickly if it is simultaneously accompanied by the sound of
its bark.
These multisensory processing regions also build up perceptions of the body as
it moves through the world, Dr. Blanke said. Sensors in the skin provide
information about pressure, pain, heat, cold and similar sensations. Sensors in
the joints, tendons and bones tell the brain where the body is positioned in
space. Sensors in the ears track the sense of balance. And sensors in the
internal organs, including the heart, liver and intestines, provide a readout of
a person’s emotional state.
Real-time information from the body, the space around the body and the
subjective feelings from the body are also represented in multisensory regions,
Dr. Blanke said. And if these regions are directly simulated by an electric
current, as in the cases of the two women he studied, the integrity of the sense
of body can be altered.
As an example, Dr. Blanke described the case of a 22-year-old student who had
electrodes implanted into the left side of her brain in 2004.
“We were checking language areas,” Dr. Blanke said, when the woman turned her
head to the right. That made no sense, he said, because the electrode was
nowhere near areas involved in the control of movement. Instead, the current was
stimulating a multisensory area called the angular gyrus.
Dr. Blanke applied the current again. Again, the woman turned her head to the
right. “Why are you doing this?” he asked.
The woman replied that she had a weird sensation that another person was lying
beneath her on the bed. The figure, she said, felt like a “shadow” that did not
speak or move; it was young, more like a man than a woman, and it wanted to
interfere with her.
When Dr. Blanke turned off the current, the woman stopped looking to the right,
and said the strange presence had gone away. Each time he reapplied the current,
she once again turned her head to try to see the shadow figure.
When the woman sat up, leaned forward and hugged her knees, she said that she
felt as if the shadow man was also sitting and that he was clasping her in his
arms. She said it felt unpleasant. When she held a card in her right hand, she
reported that the shadow figure tried to take it from her. “He doesn’t want me
to read,” she said.
Because the presence closely mimicked the patient’s body posture and position,
Dr. Blanke concluded that the patient was experiencing an unusual perception of
her own body, as a double. But for reasons that scientists have not been able to
explain, he said, she did not recognize that it was her own body she was
sensing.
The feeling of a shadowy presence can occur without electrical stimulation to
the brain, Dr. Brugger said. It has been described by people who undergo sensory
deprivation, as in mountaineers trekking at high altitude or sailors crossing
the ocean alone, and by people who have suffered minor strokes or other
disruptions in blood flow to the brain.
Six years ago, another of Dr. Blanke’s patients underwent brain stimulation to a
different multisensory area, the angular gyrus, which blends vision with the
body sense. The patient experienced a complete out-of-body experience.
When the current flowed, she said: “I am at the ceiling. I am looking down at my
legs.”
When the current ceased, she said: “I’m back on the table now. What happened?”
Further applications of the current returned the woman to the ceiling, causing
her to feel as if she were outside of her body, floating, her legs dangling
below her. When she closed her eyes, she had the sensation of doing sit-ups,
with her upper body approaching her legs.
Because the woman’s felt position in space and her actual position in space did
not match, her mind cast about for the best way to turn her confusion into a
coherent experience, Dr. Blanke said. She concluded that she must be floating up
and away while looking downward.
Some schizophrenics, Dr. Blanke said, experience paranoid delusions and the
sense that someone is following them. They also sometimes confuse their own
actions with the actions of other people. While the cause of these symptoms is
not known, he said, multisensory processing areas may be involved.
When otherwise normal people experience bodily delusions, Dr. Blanke said, they
are often flummoxed. The felt sensation of the body is so seamless, so familiar,
that people do not realize it is a creation of the brain, even when something
goes wrong and the brain is perturbed.
Yet the sense of body integrity is rather easily duped, Dr. Blanke said.
And while it may be tempting to invoke the supernatural when this body sense
goes awry, he said the true explanation is a very natural one, the brain’s
attempt to make sense of conflicting information.
Out-of-Body
Experience? Your Brain Is to Blame, NYT, 3.10.2006,
http://www.nytimes.com/2006/10/03/health/psychology/03shad.html
Federal Policy
Calling for More H.I.V. Testing
Poses a
Unique Challeng
in New York
October 2, 2006
The New York Times
By RICHARD PÉREZ-PEÑA
When it comes to H.I.V. and AIDS — the epidemic and its
politics — New York has always looked different from the rest of the country. It
has the nation’s highest rates of infection and illness, an unusual range of
public and private services for those affected, and some of the biggest and
best-organized advocacy groups.
Yet New York closely mirrors the national epidemic in some distressing ways,
including this: About one of every four new H.I.V. diagnoses comes when the
patient is found already to have AIDS. That means that in those cases, the
infection went not only untreated, but undetected for a decade, on average.
Less than two weeks ago, the federal Centers for Disease Control and Prevention
adopted a new, more aggressive policy on H.I.V. testing, saying that it should
become a routine part of doctor visits. The agency and its supporters argue that
finding more hidden infections would save lives, getting people into treatment
earlier and persuading them to change their sexual behavior and reduce the
spread of the virus.
That change, however, poses a political challenge in New York, where a state law
passed in the 1980’s to protect the rights of people with H.I.V. and AIDS makes
it impossible to carry out the new federal guidelines, which are voluntary.
While advocates agree that too few people are tested now, and that the C.D.C.
recommendations will inform a continuing debate about the state law, people on
all sides say there is no sign that the new federal policy would change things
in New York.
The debate turns on ideas about civil liberties that are balanced a little
differently in New York than in most of the country, and on widely differing
theories about why millions of people who should be tested are not.
If this dispute lacks the fierce tone of past arguments about AIDS laws, experts
say it remains more heated in New York than just about anywhere else. “We are
still the epicenter of the epidemic,” said Dr. Marjorie Hill, interim executive
director of Gay Men’s Health Crisis.
Since December, New York City’s health commissioner, Thomas R. Frieden, has made
a serious push to change the state law, but he has made little headway in
Albany. The Pataki administration has not taken sides, before or after the new
federal guidelines. Advocacy groups that strenuously oppose Dr. Frieden, along
with key lawmakers, say that nothing they have heard from him or the C.D.C. has
altered their views — at least, not yet.
“What they’re recommending would require a significant change in New York law,
and I am opposed to weakening the protections we have,” said Assemblyman Richard
N. Gottfried, a Manhattan Democrat who is chairman of his house’s health
committee.
The Senate’s health committee chairman, Kemp Hannon, a Republican from Nassau
County, said he was open to arguments that the law should change, but cautiously
so — in other words, he stands where he did all along. “I want to at least
explore it and see where we can go,” he said.
New York law requires that a doctor or anyone else ordering an H.I.V. test must
first have the patient read and sign an “informed consent” form, explaining the
test and the patient’s rights, separate from the general consent forms often
used to authorize a range of medical tests.
The law says that before the form is signed, the person ordering the test must
provide “an explanation of the nature of AIDS and H.I.V.-related illness,
information about discrimination problems that disclosure of the test result
could cause and legal protections against such discrimination, and information
about behavior known to pose risks for transmission and contraction of H.I.V.
infection.”
If a patient tests positive, the person who delivers that news is required to
provide “counseling or referrals for counseling” on the emotional effects of the
diagnosis, the discrimination that could result, and the need to change sexual
practices, among other areas.
A dozen or so states — experts disagree on the number — require specific,
informed consent for H.I.V. testing; the others do not. Adding the required
counseling before and after the test makes New York’s law one of the most
stringent in the country.
The new C.D.C. guidelines tell doctors and other medical professionals that all
adults and adolescents should be tested, and that people in high-risk groups
should be tested once a year or more.
They say that health care providers should inform patients that the tests will
be done, not ask their permission, though patients can still refuse, and that
there should be no requirements for separate written consent or counseling.
Advocates of people with AIDS lobbied hard for the state law two decades ago, at
a time when medical science offered little in the way of treatment. They argued
that testing exposed people to severe discrimination, and that fear of testing
without consent could actually dissuade people from seeing doctors. Such
arguments held little sway in most states, but they carried the day in New York.
Public health officials who support the C.D.C. recommendations contend that
things are different today, with medications keeping the virus in check for many
years. They also say that the stigma of infection is less of a concern, a claim
that advocates dispute.
A central question is why so many people still are not tested — even in New York
City, where awareness of the disease is high and testing is widely available, as
is treatment, even for those who cannot pay.
Both supporters and opponents of changing the state law say that too many
doctors simply do not suggest testing to their patients.
Dr. Frieden and others argue that doctors cannot or will not take the time to
take all the steps required by New York law to test their patients. “They have a
huge number of things that they’re supposed to cover,” he said, while pressure
from insurers to see more patients means that “they’re scrunching down to seven
or eight minutes for a single clinical encounter.”
Those who oppose changing the law insist that informed consent is not a serious
barrier, especially since the State Department of Health produced a simplified
form last year.
The problem, they say, is that doctors are uncomfortable raising the subject —
another sign of the stigma involved.
“I am an African-American woman in New York City,” part of a population at high
risk, Dr. Hill said, and yet, “I have never had a provider ask me, would I like
to take an H.I.V. test.”
Defenders of the current state law say that the way testing is handled is
crucial.
“The C.D.C. recommendations might lead to more people being tested, but is that
going to get them connected with a system of care?” said Julie Davids, executive
director of the Community H.I.V./AIDS Mobilization Project. “That connection has
to be made quickly and sensitively, or you’ll lose them, and they won’t get
treatment.”
The other side says that sensitivity matters, but that testing matters more —
after all, a person who is not tested is guaranteed not to be treated. Dr.
Frieden said studies show that people who learn that they are H.I.V.-positive
reduce behavior that could spread the virus.
“The more people who know their status, the fewer new infections you’re going to
get,” he said. “For God’s sake, people are getting sick and dying, and they
don’t have to. They’re spreading H.I.V. when they wouldn’t if they knew.”
Federal Policy
Calling for More H.I.V. Testing Poses a Unique Challenge in New York, NYT,
2.10.2006,
http://www.nytimes.com/2006/10/02/nyregion/02hiv.html
2 Americans Win
Nobel Prize in Medicine
October 2, 2006
By THE ASSOCIATED PRESS
Filed at 11:21 a.m. ET
The New York Times
STOCKHOLM, Sweden (AP) -- Americans Andrew Z. Fire and
Craig C. Mello won the Nobel Prize in medicine Monday for discovering a powerful
way to turn off the effect of specific genes, opening a potential new avenue for
fighting diseases as diverse as cancer and AIDS.
The process, called RNA interference, also is being studied for treating such
conditions as hepatitis virus infection and heart disease. It is already widely
used in basic science as a method to study the function of genes.
Fire, 47, of Stanford University, and Mello, 45, of the University of
Massachusetts Medical School in Worcester, published their seminal work in a
1998 paper.
RNA interference occurs naturally in plants, animals and humans. The Karolinska
Institute in Stockholm, which awarded the $1.4 million prize, said it is
important for regulating the activity of genes and helps defend against viral
infection. The two scientists will share the prize money.
''This year's Nobel laureates have discovered a fundamental mechanism for
controlling the flow of genetic information,'' the institute said.
Erna Moller, a member of the Nobel committee, said their research helped shed
new light on a complicated process that had confused researchers for years.
''It was like opening the blinds in the morning,'' she said. ''Suddenly you can
see everything clearly.''
Jeremy M. Berg, director of the National Institute of General Medical Sciences
in Bethesda, Md., which has funded work by Fire and Mello for years, said he
predicted the two men would win this year.
''It's an example of a discovery of a fundamental biological process that has an
almost unlimited number of implications,'' Berg said. ''The impact has just been
steadily growing.''
Genes produce their effect by sending molecules called messenger RNA to the
protein-making machinery of a cell. In RNA interference, certain molecules
trigger the destruction or inactivation of RNA from a particular gene, so that
no protein is produced. Thus the gene is effectively silenced.
For instance, a gene causing high blood cholesterol levels was recently shown to
be silenced in animals through RNA interference.
''This has been such a revolution in biomedicine, everybody is using it,'' said
Thomas Cech, president of the Howard Hughes Medical Institute, for which Mello
is an investigator.
''It's so important that people almost take it for granted already, even though
it was discovered fairly recently,'' he said.
The prize for Mello and Fire did come remarkably quickly after they did the
work. Nobels are generally given decades after the research they honor.
Mello, reached at his home in Shrewsbury, Mass., said the award came as a ''big
surprise.''
''I knew it was a possibility, but I didn't really expect it for perhaps a few
more years. Both Andrew and I are fairly young, 40 or so, and it's only been
about eight years since the discovery.''
He said he would try to get to work Monday but expected to accomplish ''not a
lot.''
Fire, reached in California, said he was awakened by a call from the Nobel
committee.
`At first I was very excited.... Then I thought I must be dreaming or maybe it
was the wrong number,'' he said. But then he confirmed the good news by checking
the Nobel Web site.
''It makes me feel great. It makes me feel incredibly indebted at the same
time,'' he said. ''You realize how many other people have been major parts of
our efforts.''
Fire conducted his research while at the Washington-based Carnegie Institution.
The announcement opened this year's series of prize announcements. It will be
followed by Nobel prizes for physics, chemistry, literature, peace and
economics.
Last year's medicine prize went to Australians Barry J. Marshall and Robin
Warren for discovering that bacteria, not stress, causes ulcers.
Alfred Nobel, the Swedish inventor of dynamite, established the prizes in his
will in the categories of literature, peace, medicine, physics and chemistry.
The economics prize is technically not a Nobel but a 1968 creation of Sweden's
central bank.
Winners receive a check, handshakes with Scandinavian royalty, and a banquet on
Dec. 10 -- the anniversary of Nobel's death in 1896. All prizes are handed out
in Stockholm except for the peace prize, which is presented in Oslo.
On the Net:
Nobel Foundation: http://nobelprize.org/
2 Americans Win
Nobel Prize in Medicine, NYT, 2.10.2006,
http://www.nytimes.com/aponline/world/AP-Nobel-Medicine.html
Hope, at $4,200 a Dose
October 1, 2006
The New York Times
By ALEX BERENSON
CHARGING $4,200 a dose for a new version of an old cancer
drug has helped make Dr. Patrick Soon-Shiong a billionaire.
The drug, Abraxane, does not help patients live longer than the older treatment,
though it does shrink tumors in more patients, according to clinical trials. And
the old and new medicines have similar side effects. An independent review of
Abraxane published in December in a cancer research journal concluded that the
drug was “old wine in a new bottle.”
Still, Dr. Soon-Shiong’s company, Abraxis BioScience, has promoted Abraxane as a
major advance in treating late-stage breast cancer — that is, for patients who
have not responded to other treatments and are now close to death — and is
seeking approval for patients to use it earlier in their treatment. And, in at
least one way, Abraxane is a breakthrough: it costs about 25 times as much as a
generic version of the older medicine, which is best known by its brand name,
Taxol.
Because of the odd economics of the cancer drug market, though, Abraxane’s price
does not seem to be hurting its popularity.
About 20,000 people have now been treated with the drug, and Dr. Soon-Shiong
expects its sales to approach $200 million this year. By 2010, Abraxane’s annual
sales could reach $1 billion, analysts say.
Those rosy forecasts illustrate the pricing power that makers of cancer drugs
wield. With patients often facing grim prognoses and desperate for new
therapies, and insurers relatively powerless to negotiate prices or deny
coverage, the cost of treatments seems to have little impact on demand.
The rise in cancer-drug prices is a microcosm of broader trends pushing up
health care costs nationally. Despite decades of efforts by governments and
insurers to restrain costs, patients continue to want the newest — and most
expensive — drugs and medical devices. And doctors and the health care industry
have little reason to keep costs in check, because insurers rarely deny coverage
for new treatments on the basis of price.
As a result, health care costs continue to skyrocket. On Tuesday, the Kaiser
Family Foundation reported that the cost of employee health insurance coverage
rose 8 percent, according to a survey conducted from January to May this year.
Businesses now spend about $8,500 a year for health insurance for the average
family, the foundation said, with employees adding $3,000, not counting the cost
of deductibles and other out-of-pocket payments.
Abraxane, and cancer drugs generally, are still a tiny part of total medical
spending. But their costs are rising even faster than overall health care
inflation. Worldwide, spending on cancer drugs is expected to more than double
from 2004 to 2009, to $55 billion, with most of that in the United States.
LARGELY as a result of investor enthusiasm for Abraxane, the stock market value
of Abraxis is $4.6 billion.The company, which also makes several generic drugs
used in hospitals, had a profit of $86 million last year on sales of $519
million. Dr. Soon-Shiong, the company’s chairman, owns 84 percent of the stock,
worth about $3.8 billion.
Dr. Soon-Shiong, a Los Angeles surgeon with a controversial history in the drug
industry, says Abraxane’s price is justified because it causes fewer allergic
reactions than Taxol, whose chemical name is paclitaxel. And his company is
spending large sums on clinical trials to test Abraxane in new categories of
cancer patients, he said.
“We have a breakthrough,” he said. “Look at the data.”
Dr. Soon-Shiong also noted that although Abraxane has not been proved to prolong
survival, it does appear to cause tumors to shrink more often than does Taxol.
In the clinical trial that led to Abraxane’s approval, about 24 percent of
patients showed some response to Abraxane, compared with 11 percent for Taxol.
Independent oncologists agree that reducing the risk of allergic reactions is an
advantage — and perhaps reason enough for doctors to choose Abraxane, costs
aside. Still, in clinical trials, Abraxane’s overall side-effect profile was
similar to that of paclitaxel, which was approved as a chemotherapy treatment in
1992 and is still widely used. Both Abraxane and Taxol can kill white blood
cells, leaving patients open to infection, as well as damage nerves in the hands
and feet. Taxol causes more damage to white blood cells, while Abraxane causes
more nerve damage.
Drug industry experts say Abraxane’s price reflects the fact that makers of
cancer drugs can charge high prices for new medicines even if they are only
marginally better than their older counterparts. That pricing dynamic is enabled
by insurance, which shields patients from the full price of drugs. Without
pressure from their insurers, patients have little reason to choose older
treatments over expensive new therapies.
Doctors, who ultimately decide what drugs to prescribe, also do not have to
worry about paying for the treatments they choose.
“When I’m with a patient, my job is to be a patient advocate, not to try to save
society money on chemotherapy,” said Dr. Barbara L. McAneny, the chief executive
of New Mexico Oncology/Hematology Consultants, in Albuquerque.
The Food and Drug Administration, meanwhile, does not regulate drug prices but
considers only whether new medicines are safe and effective. Medicare, which
pays for Abraxane, is also forbidden by law from considering cost in deciding
what treatments to cover.
While insurers have tried to save money in other drug categories by encouraging
patients to use cheaper generic drugs, they face public pressure not to restrict
access to new cancer treatments. At least since 1971, when President Richard M.
Nixon declared a “war on cancer” and vowed to eliminate it, cancer has been
viewed as a uniquely frightening disease that deserves the highest priority for
research and treatment.
At the same time, most cancer drugs cannot be easily substituted for one
another, preventing insurers from playing one drug maker against a rival to
achieve lower prices. Abraxis, despite having a close generic competitor for its
drug, appears to be benefiting from the insurance industry’s acquired habit of
paying for whatever the cancer doctor prescribes.
“Everyone is well aware that prices keep going up,” said Dr. Steven B. Miller,
the chief medical officer at CuraScript, a division of Express Scripts, which
helps companies manage their drug insurance plans. But employers are reluctant
to tell Express Scripts to refuse to pay for costly new cancer drugs, Dr. Miller
said.
“Do you want your employees calling and saying, ‘You’re denying my family the
latest cancer care?’ ” Dr. Miller said. “Until the payor community” — that is,
companies that provide health insurance — “develops the appetite to be more
aggressive, it would be irresponsible for us to press them on it,” he added.
But Dr. John C. Hornberger, a senior research associate at the Sphere Institute,
a nonprofit health and public policy group in Burlingame, Calif., says employers
are wary of interfering in medical decision-making by their employees. “They
want to control costs,” he said, “but they don’t want to be involved.”
Carol Austin-Fink, who learned last year that she had cancer in her right
breast, insisted on taking Abraxane after she received the diagnosis because the
chemotherapy she received in 1996 for a different cancer in her left breast had
caused severe side effects. The earlier treatment did not include Taxol, so she
had no idea whether Taxol would cause problems for her, but she did not want to
take the chance.
Ms. Austin-Fink, a 59-year-old writer who lives in Las Vegas, said she received
six doses of Abraxane over four months, a standard course of treatment. The cost
of the drug did not concern her because she has excellent insurance coverage,
she said.
“My insurance company just paid it, because my doctors said they needed it, and
the insurance company doesn’t argue with stuff like that,” Ms. Austin-Fink said.
The Abraxane had few side effects and caused her tumor to shrink almost
immediately. Her cancer has remained under control since her final treatment a
year ago, she said. She said she believes that Abraxane worked better for her
than Taxol would have, though she acknowledged that she could not be sure.
Drug companies have sharply increased prices for new cancer drugs in the last
decade. Since 1998, for example, Celgene, a biotechnology company based in
Summit, N.J., has raised the price of Thalomid, a drug for a cancer called
multiple myeloma, to more than $35,000 a year from $4,000.
Celgene is not alone. New treatments now routinely cost several thousand dollars
a month. Worldwide spending on cancer medicines, which was $24 billion in 2004,
is expected to rise to $55 billion in 2009, making oncology treatments the
biggest drug category, according to IMS Health, which provides data on drug
sales.
The higher prices are beginning to strain the system, said Carolina Hinestrosa,
executive vice president at the National Breast Cancer Coalition, an advocacy
group.
Even if they have insurance, many patients face co-payments of 20 percent for
their cancer drugs, an expense that can become ruinous for patients receiving
combination therapy with several new drugs. For example, Abraxane is being
tested along with Avastin, a treatment from Genentech that costs $8,000 a month
for some patients.
Drug costs are rising so fast that some patients cannot afford the newest
treatments, and access to some therapies “is beginning to be eroded,” Ms.
Hinestrosa said.
ORIGINALLY, Taxol itself was considered expensive. When the F.D.A. approved it
in December 1992, its price of $986 a dose led to Congressional hearings. Since
2000, when Bristol-Myers Squibb’s patent on Taxol expired, the drug has been
available both as nonbranded generic paclitaxel and as branded Taxol, at a cost
of about $150 a dose for the generic and $1,000 for the branded version, which
is now sold mostly outside the United States.
These days, though, high prices rarely draw public protests, in part because
most patients are still receiving their medicines. That is accomplished through
a mix of insurance coverage and programs sponsored by charities and drug makers,
including Abraxis, that provide free supplies to the indigent.
“There isn’t an effort in terms of public policy to keep prices under control,”
Ms. Hinestrosa said.
Megan Murphy, an analyst at Lazard Capital Markets who follows Abraxis, agrees.
While doctors and patients have begun to complain, drug makers still have
substantial pricing power, she said. “At some point, something will change
here,” she said. “But there doesn’t seem to be any real resistance right now.”
Dr. Soon-Shiong said in an interview that he, too, worried about the cost of
cancer treatment. But Abraxane is fairly priced, he said, because it is based on
a scientific breakthrough that the company refers to as “nanoparticle
technology.”
This is not the first time that Dr. Soon-Shiong has aggressively promoted a new
disease treatment. In the mid-1990’s, he won attention for transplanting
pancreatic cells into two diabetic patients. Eventually, the transplants failed.
At about the same time that Dr. Soon-Shiong was researching both diabetes
treatments and Abraxane, he created a company called American Pharmaceutical
Partners to market generic drugs to hospitals. American Pharmaceutical generated
controversy by giving stock options to executives at a company responsible for
buying drugs on behalf of hospitals nationwide. Some doctors said the stock
options created a serious conflict of interest by giving the executives — who
were supposed to represent the hospitals — a financial interest in American
Pharmaceutical’s success. American Pharmaceutical denied any wrongdoing and said
all the arrangements were properly disclosed.
Dr. Soon-Shiong created Abraxis BioScience earlier this year by merging American
Pharmaceutical Partners with another company he controlled, American BioScience.
Shareholders in American Pharmaceutical Partners have sued him over the merger,
contending that it benefited him at their expense. Dr. Soon-Shiong says that he
has done nothing wrong and that the lawsuits are irrelevant to Abraxane’s
promise.
ABRAXANE is a reformulated version of paclitaxel, a chemical found in the
Pacific yew tree that destroys cancer cells. But paclitaxel, which is given
intravenously, is difficult to use. Because it does not dissolve in water, the
drug must be mixed in Cremophor, a combination of castor oil and alcohol that
can cause severe allergic reactions. To reduce that risk, patients who receive
Cremophor first receive a steroid and an antihistamine.
Working with University of Illinois researchers in the 1990’s, Dr. Soon-Shiong
found a way to give Taxol without Cremophor by coating paclitaxel in fragments
of albumin, a protein found in human blood. He named the new treatment Abraxane.
Abraxane patients do not need antihistamines or steroids. The drug can also be
given at slightly higher doses and injected more quickly than traditional
paclitaxel, which requires a three hour-infusion.
A third drug, called Taxotere, works similarly to paclitaxel but is a different
chemical compound; it competes with both Abraxane and Taxol. Made by
Sanofi-Aventis, Taxotere costs $2,500 a dose. It increases survival slightly in
breast cancer patients, compared with Taxol. But because Taxotere has even more
severe side effects, many patients and doctors prefer Taxol. Both drugs are
widely used. There is no published data comparing Abraxane and Taxotere.
In the largest clinical trial comparing Abraxane and Taxol, covering 454
patients, the two drugs produced similar side effects — although Taxol caused
more patients to have low white blood cell counts.
The trial also showed that Abraxane delayed the growth of tumors for 23 weeks in
the average patient, compared with 17 weeks for Taxol. That difference was
statistically significant, meaning that it probably did not occur by chance. But
the trial did not show that Abraxane extended patients’ lives longer than Taxol
did, and that is the most important measure of effectiveness. After two years,
roughly 75 percent of patients in the study had died, whether they received
Abraxane or Taxol.
Over all, Abraxane may be slightly more effective than Taxol, and the lack of
Cremophor is an advantage, said Dr. Andrew D. Seidman, a breast cancer
specialist at Memorial Sloan-Kettering Cancer Center in Manhattan who has
studied Taxol and Taxotere since the early 1990’s. But the two drugs are
similar, he said. “Is this a breakthrough in terms of the notion that this is a
new class of drug with a new mechanism of action?” he asked rhetorically. “No.”
Dr. Ramaswamy Govindan, a Washington University professor who was co-author of a
December article in the Annals of Oncology about Abraxane and other, as-yet-
unapproved Cremophor-free versions of Taxol, said that none of the new drugs had
shown significant advantages over the older medicine.
“In general, the novel formulations so far have not stood out as distinctly
superior,” Dr. Govindan said.
The F.D.A. approved Abraxane as a last-ditch treatment for late-stage breast
cancer in January 2005. Now Abraxis is asking the F.D.A. to allow the use of
Abraxane as a treatment for early-stage breast cancer, a larger market than that
for late-stage treatments. In an unusual move, the company asked the agency
earlier this year to waive its typical requirement that the drug be tested in
those patients before allowing the expanded use.
On Sept. 7, the F.D.A. convened a panel of experts in Silver Spring, Md., to
discuss Abraxis’s request.
Committee members voted against the company’s proposal 13 to 1, saying that
Abraxis needed more data. The company expects to begin discussions soon with the
F.D.A. about designing a clinical trial to test Abraxane in early-stage
patients.
At the Sept. 7 hearing, though, Dr. Michael Hawkins, Abraxis’s top medical
officer, made a remarkable observation about how the company’s $4,200-a-dose
drug compared with $150 generic paclitaxel.
Dr. Hawkins said the F.D.A. should approve Abraxane in early-stage patients
without a clinical trial because such testing would probably not prove that his
company’s drug was different than the conventional treatment. “These are just
two forms of paclitaxel,” he said.
Hope, at $4,200 a
Dose, NYT, 1.10.2006,
http://www.nytimes.com/2006/10/01/business/yourmoney/01drug.html
|