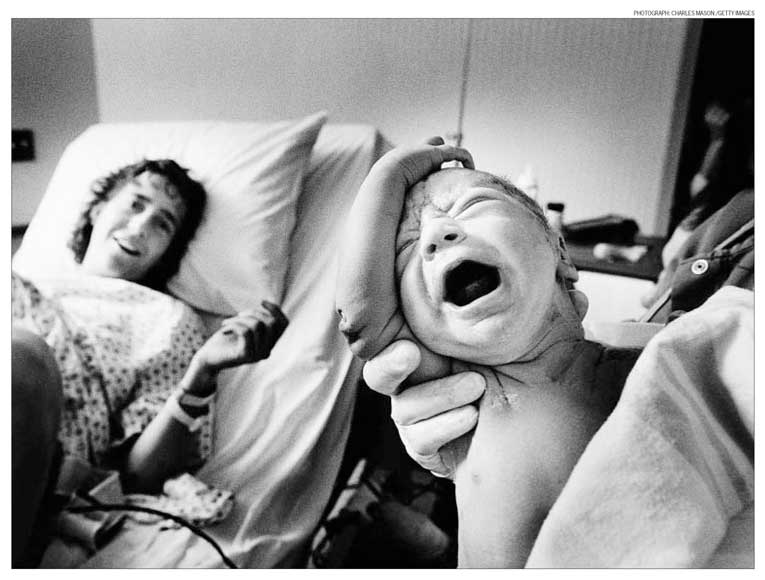
ATLANTA — FIFTY years ago this Wednesday, Americans were
gripped by the fate of a baby — Patrick Bouvier Kennedy, the first child born to
a sitting president since the 19th century, and John F. Kennedy’s last. He
arrived on Aug. 7, 1963, five and a half weeks premature. Despite medical
heroics, including the use of a hyperbaric oxygen chamber, he died 39 hours
later.
Neonatal care has improved greatly since then. Were he born today, Patrick, who
was delivered at 34 weeks’ gestation, would very likely survive and have a
healthy life, too.
For all the biomedical advances, though, the key ethical problems surrounding
premature birth remain. Today, babies as much as 11 weeks younger than Patrick
can be saved at birth. The problem is that their prognoses are often much worse
than his would have been.
I am a neonatologist. I save babies. Most of them, especially those born after
28 weeks, will at most suffer mild or moderate disabilities. But of those born
before 28 weeks — 30,000 of the half million babies born prematurely each year
in this country — many will have serious physical, social or cognitive problems.
Consider that a one-pound, one-ounce girl born unexpectedly at 23 weeks’
gestation has a 92 percent chance of dying early or having moderate to severe
neurodevelopmental impairment.
Most extremely premature babies will experience at least one complication —
bleeding in the brain, infections, intestinal perforation, severe lung damage —
before discharge. Many will need treatment long after birth, sometimes for life,
at great financial and emotional cost to them and those around them.
A few months ago I cared for just such a child. Let’s call her Miracle. She was
born at 23 weeks’ gestation and weighed a little over a pound. Despite the bleak
prognosis, her parents asked that we resuscitate her in the delivery room.
So we did. But over the next eight weeks, to keep her alive, we had to prick
Miracle’s heel so many times she developed scarring. We suctioned her trachea
hundreds of times. We put tubes through her mouth and into her stomach, we
stabbed her again and again to insert IVs, and we took blood from her and then
transfused blood back. We gave her antibiotics for two severe infections.
Each of these events created suffering, for Miracle and her parents. Her mother
visited daily and developed an anxiety disorder. Her father came in only once a
week, the pain and sadness was so great.
After eight weeks, Miracle came off the ventilator we had put her on. But three
days later we had to turn it back on, and it was possible she would die or
remain on the ventilator permanently if we didn’t give her steroids, which can
have side effects as serious as cerebral palsy. Her mother opted for the
steroids. But Miracle’s father was angry. He muttered to me: “Why do you do
this? Why do you keep these babies alive?”
I’ve been thinking about that question for decades and haven’t found a simple
answer. Some parents believe that withholding or withdrawing life-sustaining
treatment will prevent their infant from suffering and living a life not worth
living; others consider it murder. Some families soar in caring for their
disabled kids; others disintegrate.
Ultimately, parents have the right to decide, but we physicians must help them
make informed decisions. I asked Miracle’s father whether anyone had talked to
him about resuscitating Miracle before she was born. He vaguely remembered a
conversation, but hadn’t understood what treating such a tiny premature baby
meant.
And nobody talked to him after Miracle was born about continuing life-sustaining
treatment. In fact, he had gotten to her two-month birthday without realizing
that her suffering might end in death. We had updated his wife, but she didn’t
like to hear bad news, and didn’t tell him.
Luckily, the news has improved. Miracle is off the ventilator and will likely
survive to be discharged, though she will suffer from chronic lung disease.
Even so, we need to make sure both parents are always kept part of the
discussion, to ensure we have their informed consent throughout treatment. It
can’t be just one conversation.
More broadly, when in the first trimester obstetricians talk with pregnant women
and their partners about testing for genetic anomalies, they should include
discussion of values and attitudes toward life, death and disability, or at
least recommend such discussions. Certainly parents at high risk of giving birth
to premature babies, or to babies with severe congenital defects, should receive
such counseling, including from neonatologists and other specialists.
Sometimes, I think we doctors need to do more than inform. On occasion, I’ve
offered to make a life-or-death decision for parents. If they agree, they are
essentially making the decision, but are shifting the burden to me. It’s harder
for parents to say, “I unplugged my baby,” than to let the doctor do it.
Our culture is slowly growing more comfortable talking about end-of-life issues
as they relate to the elderly: whether to allow a natural death or prolong life
even if it means suffering.
In my world, though, the “surrogate” decision makers are young parents of
infants like Miracle. And they are still completely unprepared. It’s time we
broaden the discussion to include them.
A wave of mergers between Roman Catholic and secular hospitals is threatening to
deprive women in many areas of the country of ready access to important
reproductive services. Catholic hospitals that merge or form partnerships with
secular hospitals often try to impose religious restrictions against abortions,
contraception and sterilization on the whole system.
This can put an unacceptable burden on women, especially low-income women and
those who live in smaller communities where there are fewer health care options.
State regulators should closely examine such mergers and use whatever powers
they have to block those that diminish women’s access to medical care.
Gov. Steve Beshear of Kentucky, for example, recently turned down a bid by a
Catholic health system to merge with a public hospital that is the chief
provider of indigent care in Louisville. He cited concerns about loss of control
of a public asset and restrictions on reproductive services.
The nation’s 600 Catholic hospitals are an important part of the health care
system. They treat one-sixth of all hospital patients, and are sometimes the
only hospital in a small community. They receive most of their operating income
from public insurance programs like Medicare and Medicaid and from private
insurers, not from the Catholic Church. They are free to deliver care in accord
with their religious principles, but states and communities have an obligation
to make sure that reproductive care remains available. This should be a central
goal for government officials who have a role in approving such consolidations.
As Reed Abelson wrote in a recent report in The Times, these mergers are driven
by shifts in health care economics. Some secular hospitals are struggling to
survive and eager to be rescued by financially stronger institutions, which in
many cases may be Catholic-affiliated. By one estimate, 20 mergers between
Catholic and non-Catholic hospitals have been announced over the past three
years and more can be expected.
The 2009 “Ethical and Religious Directives” issued by the United States
Conference of Catholic Bishops warns that Catholic institutions should avoid
entering into partnerships “that would involve them in cooperation with the
wrongdoing of other providers.” Catholic hospitals have refused to terminate
pregnancies, provide contraceptive services, offer a standard treatment for
ectopic pregnancies, or allow sterilization after caesarean sections (women
seeking tubal ligations are then forced to have a second operation elsewhere,
exposing them to additional risks).
In one case, the sole hospital in a rural area in southeastern Arizona announced
in 2010 that it would partner with an out-of-state Catholic health system, and
would immediately adhere to Catholic directives that forbid certain reproductive
health services. As a result, a woman whose doctors wanted to terminate a
pregnancy to save her life had to be sent 80 miles away for treatment. A
coalition of residents, physicians and activists campaigned against the merger
and it was called off before it was finalized.
Over the past 15 years, MergerWatch, an advocacy group based in New York City,
has helped block or reverse 37 mergers and reached compromises in 22 others that
saved at least some reproductive services. As mergers become more common, state
and local leaders would be wise to block proposals that restrict health
services.
AMID the sound and fury of the latest culture-war battles —
first over breast cancer dollars and Planned Parenthood, and then over the White
House’s attempt to require that religious employers cover contraception and
potential abortifacients — it’s easy to forget that there is at least some
common ground in American politics on sex, pregnancy, marriage and abortion.
Even the most pro-choice politicians, for instance, usually emphasize that they
want to reduce the need for abortion, and make the practice rare as well as safe
and legal. Even the fiercest conservative critics of the White House’s
contraception mandate — yes, Rick Santorum included — agree that artificial
birth control should be legal and available. And both Democrats and Republicans
generally agree that the country would be better off with fewer pregnant
teenagers, fewer unwanted children, fewer absent fathers, fewer out-of-wedlock
births.
Where cultural liberals and social conservatives differ is on the means that
will achieve these ends. The liberal vision tends to emphasize access to
contraception as the surest path to stable families, wanted children and low
abortion rates. The more direct control that women have over when and whether
sex makes babies, liberals argue, the less likely they’ll be to get pregnant at
the wrong time and with the wrong partner — and the less likely they’ll be to
even consider having an abortion. (Slate’s Will Saletan has memorably termed
this “the pro-life case for Planned Parenthood.”)
The conservative narrative, by contrast, argues that it’s more important to
promote chastity, monogamy and fidelity than to worry about whether there’s a
prophylactic in every bedroom drawer or bathroom cabinet. To the extent that
contraceptive use has a significant role in the conservative vision (and
obviously there’s some Catholic-Protestant disagreement), it’s in the context of
already stable, already committed relationships. Monogamy, not chemicals or
latex, is the main line of defense against unwanted pregnancies.
The problem with the conservative story is that it doesn’t map particularly well
onto contemporary mores and life patterns. A successful chastity-centric culture
seems to depend on a level of social cohesion, religious intensity and shared
values that exists only in small pockets of the country. Mormon Utah, for
instance, largely lives up to the conservative ideal, with some of America’s
lowest rates of teenage pregnancies, out-of-wedlock births and abortions. But
many other socially conservative regions (particularly in the South) feature
higher rates of unwed and teenage parenthood than in the country as a whole.
Liberals love to cite these numbers as proof that social conservatism is a flop.
But the liberal narrative has glaring problems as well. To begin with, a lack of
contraceptive access simply doesn’t seem to be a significant factor in unplanned
pregnancy in the United States. When the Alan Guttmacher Institute surveyed more
than 10,000 women who had procured abortions in 2000 and 2001, it found that
only 12 percent cited problems obtaining birth control as a reason for their
pregnancies. A recent Centers for Disease Control and Prevention study of
teenage mothers found similar results: Only 13 percent of the teens reported
having had trouble getting contraception.
At the same time, if liberal social policies really led inexorably to fewer
unplanned pregnancies and thus fewer abortions, you would expect “blue” regions
of the country to have lower teen pregnancy rates and fewer abortions per capita
than demographically similar “red” regions.
But that isn’t what the data show. Instead, abortion rates are frequently higher
in more liberal states, where access is often largely unrestricted, than in more
conservative states, which are more likely to have parental consent laws,
waiting periods, and so on. “Safe, legal and rare” is a nice slogan, but liberal
policies don’t always seem to deliver the “rare” part.
What’s more, another Guttmacher Institute study suggests that liberal states
don’t necessarily do better than conservative ones at preventing teenagers from
getting pregnant in the first place. Instead, the lower teenage birth rates in
many blue states are mostly just a consequence of (again) their higher abortion
rates. Liberal California, for instance, has a higher teen pregnancy rate than
socially conservative Alabama; the Californian teenage birth rate is only lower
because the Californian abortion rate is more than twice as high.
These are realities liberals should keep in mind when tempted to rail against
conservatives for rejecting the intuitive-seeming promise of “more condoms,
fewer abortions.” What’s intuitive isn’t always true, and if social
conservatives haven’t figured out how to make all good things go together in
post-sexual-revolution America, neither have social liberals.
At the very least, American conservatives are hardly crazy to reject a model for
sex, marriage and family that seems to depend heavily on higher-than-average
abortion rates. They’ve seen that future in places like liberal, cosmopolitan
New York, where two in five pregnancies end in abortion. And it isn’t a pretty
sight.